

Existence and functionality of emergency obstetric care services at district level in Kenya: theoretical coverage versus reality
- PMID: 23522087
- PMCID: PMC3616893
- DOI: 10.1186/1472-6963-13-113
Existence and functionality of emergency obstetric care services at district level in Kenya: theoretical coverage versus reality
Abstract
Background: The knowledge on emergency obstetric care (EmOC) is limited in Kenya, where only partial data from sub-national studies exist. The EmOC process indicators have also not been integrated into routine health management information system to monitor progress in safe motherhood interventions both at national and lower levels of the health system. In a country with a high maternal mortality burden, the implication is that decision makers are unaware of the extent of need for life-saving care and, therefore, where to intervene. The objective of the study was to assess the actual existence and functionality of EmOC services at district level.
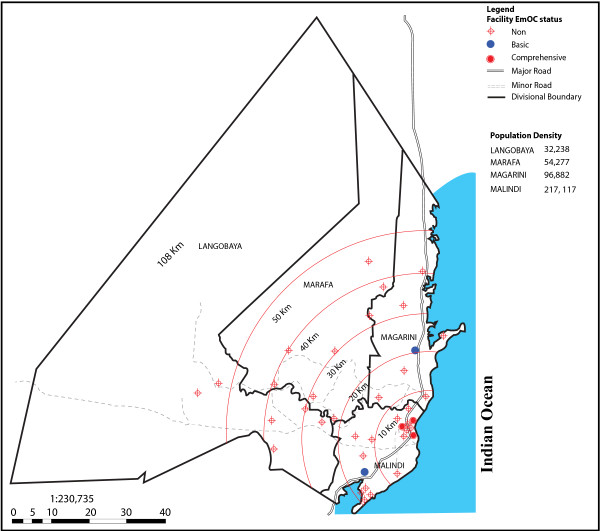
Methods: This was a facility-based cross-sectional study. Data were collected from 40 health facilities offering delivery services in Malindi District, Kenya. Data presented are part of the "Response to accountable priority setting for trust in health systems" (REACT) study, in which EmOC was one of the service areas selected to assess fairness and legitimacy of priority setting in health care. The main outcome measures in this study were the number of facilities providing EmOC, their geographical distribution, and caesarean section rates in relation to World Health Organization (WHO) recommendations.
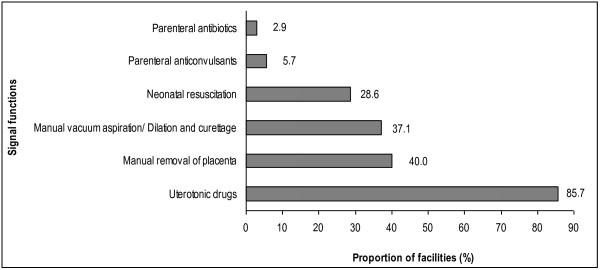
Results: Among the 40 facilities assessed, 29 were government owned, seven were private and four were voluntary organisations. The ratio of EmOC facilities to population size was met (6.2/500,000), compared to the recommended 5/500,000. However, using the strict WHO definition, none of the facilities met the EmOC requirements, since assisted delivery, by vacuum or forceps was not provided in any facility. Rural-urban inequities in geographical distribution of facilities were observed. The facilities were not providing sufficient life-saving care as measured by caesarean section rates, which were below recommended levels (3.7% in 2008 and 4.5% in 2009). The rates were lower in the rural than in urban areas (2.1% vs. 6.8%; p < 0.001 ) in 2008 and (2.7% vs. 7.7%; p < 0.001) in 2009.
Conclusions: The gaps in existence and functionality of EmOC services revealed in this study may point to the health system conditions contributing to lack of improvements in maternal survival in Kenya. As such, the findings bear considerable implications for policy and local priority setting.
Figures
References
-
- Kenya National Bureau of Statistics, ICF Macro. Kenya Demographic and Health Survey 2008–09. Calverton, Maryland: Kenya National Bureau of Statistics, ICF Macro; 2010.
-
- WHO, UNICEF, UNFPA and the World Bank. Trends in maternal mortality 1990–2008: estimates developed by WHO, UNICEF, UNFPA and The World Bank. Geneva: World Health Organization; 2010.
-
- UON Network. Tackling Unmet Needs for Major Obstetric Interventions. Part 1: Concepts, General Principles and International Network. [ http://www./uonn.org/pdf/Guide1.pdf]. Accessed March 2013.
-
- Koblinsky MA. Reducing Maternal Mortality. Learning from Bolivia, China, Egypt, Honduras, Indonesia, Jamaica, and Zimbabwe. Washington, D.C: The World Bank; 2003.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
