

Factors to inform clinicians about the end of life in severe chronic obstructive pulmonary disease
- PMID: 23522520
- PMCID: PMC3728164
- DOI: 10.1016/j.jpainsymman.2012.10.283
Factors to inform clinicians about the end of life in severe chronic obstructive pulmonary disease
Abstract
Context: Palliative services have historically been offered to terminal patients with cancer, but much less so in other chronic illnesses such as chronic obstructive pulmonary disease (COPD) because of difficulties in predicting the trajectory to death.
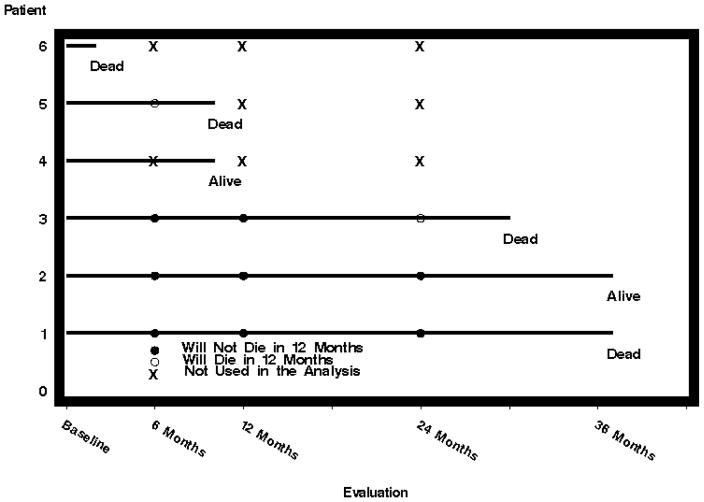
Objectives: The goal of this study was to determine if the change over time of the key parameters (trajectory) in patients with severe COPD can independently predict short-term mortality.
Methods: We analyzed data from 1218 patients with severe COPD. Multivariate models for trajectory change were used to forecast mortality at 12 months.
Results: Changes in several variables by defined cutpoints increase significantly and independently the odds of dying in 12 months. The earliest and strongest predictors were the decrease in gait speed by 0.14 m/s or six-minute walk by 50 m (odds ratio [OR] 4.40, P<0.0001). Alternatively, if six-minute walk or gait speed were not used, change toward perceiving a very sedentary state using a single question (OR 3.56, P=0.0007) and decrease in maximal inspiratory pressure greater than 11 cmH2O (OR 2.19, P=0.0217) were predictive, followed by change toward feeling upset or downhearted (OR 2.44, P=0.0250), decrease in room air resting partial pressure of oxygen greater than 5 mmHg (OR 2.46, P=0.0156), and increase in room air resting partial pressure of carbon dioxide greater than 3 mmHg (OR 2.8, P=0.0039). Change over time models were more discriminative (higher c-statistics) than change from baseline models.
Conclusion: The changes in defined variables and patient-reported outcomes by defined cutpoints were independently associated with increased 12-month mortality in patients with severe COPD. These results may inform clinicians when to initiate end-of-life communications and palliative care.
Keywords: Chronic obstructive pulmonary disease; end-of-life care; end-stage COPD; gait speed; mortality; palliative care; prediction tools; severe COPD.
Copyright © 2013 U.S. Cancer Pain Relief Committee. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Abrahm JL, Hansen-Flaschen J. Hospice care for patients with advanced lung disease. Chest. 2002;121:220–229. - PubMed
-
- Elkington H, White P, Addington-Hall J, Higgs R, Pettinari C. The last year of life of COPD: a qualitative study of symptoms and services. Respir Med. 2004;98:439–445. - PubMed
-
- Lanken PN, Terry PB, Delisser HM, et al. An official American Thoracic Society clinical policy statement: palliative care for patients with respiratory diseases and critical illnesses. Am J Respir Crit Care Med. 2008;177:912–927. - PubMed
-
- Thorns A, Cawley D. Palliative care in people with chronic obstructive pulmonary disease. BMJ. 2011;342:d106. - PubMed
Publication types
MeSH terms
Grants and funding
- 1R01CA163293-01/CA/NCI NIH HHS/United States
- N01 HR076103/HL/NHLBI NIH HHS/United States
- N01 HR076102/HL/NHLBI NIH HHS/United States
- N01 HR076113/HL/NHLBI NIH HHS/United States
- N01 HR076104/HL/NHLBI NIH HHS/United States
- N01 HR076110/HL/NHLBI NIH HHS/United States
- N01 HR076112/HL/NHLBI NIH HHS/United States
- N01 HR076109/HL/NHLBI NIH HHS/United States
- N01 HR076105/HL/NHLBI NIH HHS/United States
- N01 HR076118/HL/NHLBI NIH HHS/United States
- N01 HR076115/HR/NHLBI NIH HHS/United States
- N01 HR076107/HL/NHLBI NIH HHS/United States
- N01 HR076106/HL/NHLBI NIH HHS/United States
- R01 CA163293/CA/NCI NIH HHS/United States
- K23 CA106544/CA/NCI NIH HHS/United States
- N01 HR076114/HL/NHLBI NIH HHS/United States
- R01 HL094680/HL/NHLBI NIH HHS/United States
- N01 HR076101/HL/NHLBI NIH HHS/United States
- N01 HR076119/HL/NHLBI NIH HHS/United States
- N01 HR076108/HL/NHLBI NIH HHS/United States
- N01 HR076116/HL/NHLBI NIH HHS/United States
- N01 HR076111/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
