

Exercise training for blood pressure: a systematic review and meta-analysis
- PMID: 23525435
- PMCID: PMC3603230
- DOI: 10.1161/JAHA.112.004473
Exercise training for blood pressure: a systematic review and meta-analysis
Abstract
Background: We conducted meta-analyses examining the effects of endurance, dynamic resistance, combined endurance and resistance training, and isometric resistance training on resting blood pressure (BP) in adults. The aims were to quantify and compare BP changes for each training modality and identify patient subgroups exhibiting the largest BP changes.
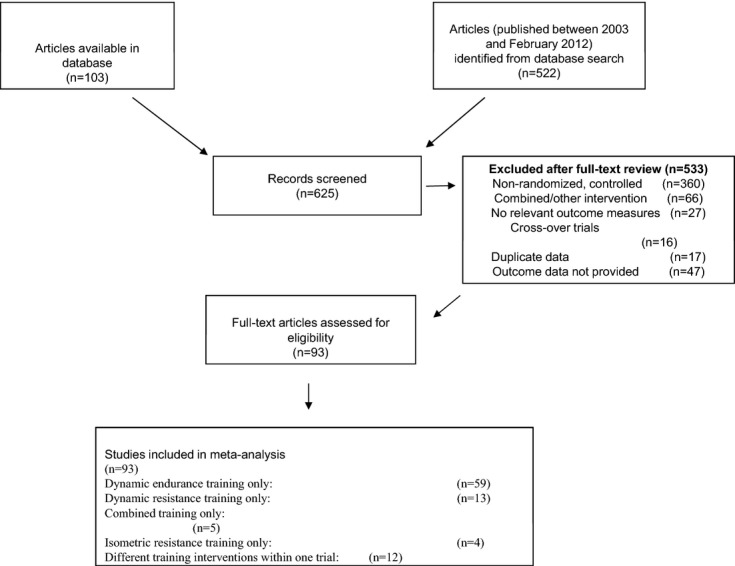
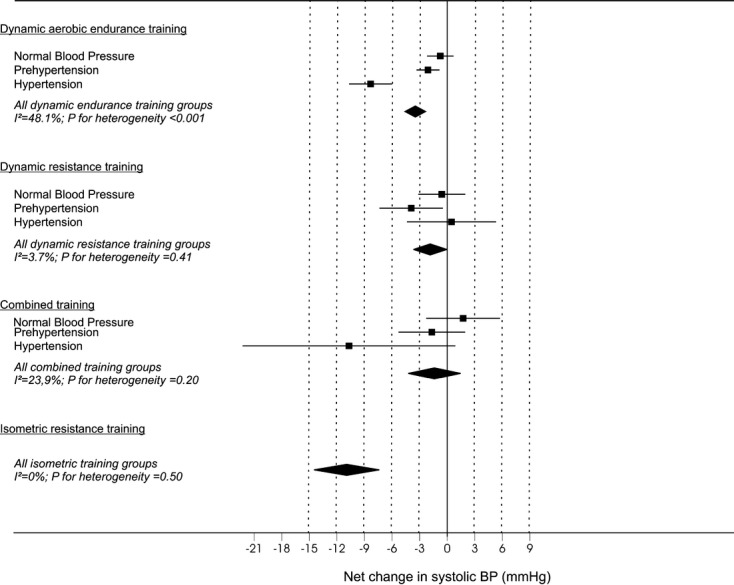
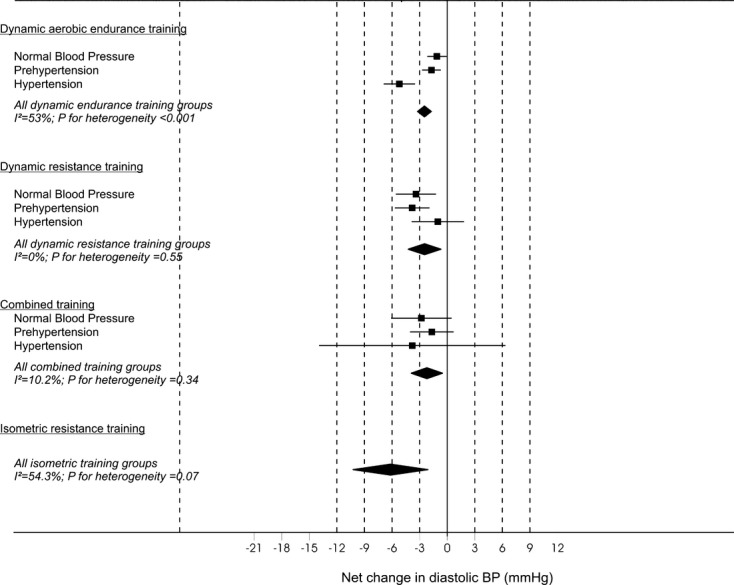
Methods and results: Randomized controlled trials lasting ≥4 weeks investigating the effects of exercise on BP in healthy adults (age ≥18 years) and published in a peer-reviewed journal up to February 2012 were included. Random effects models were used for analyses, with data reported as weighted means and 95% confidence interval. We included 93 trials, involving 105 endurance, 29 dynamic resistance, 14 combined, and 5 isometric resistance groups, totaling 5223 participants (3401 exercise and 1822 control). Systolic BP (SBP) was reduced after endurance (-3.5 mm Hg [confidence limits -4.6 to -2.3]), dynamic resistance (-1.8 mm Hg [-3.7 to -0.011]), and isometric resistance (-10.9 mm Hg [-14.5 to -7.4]) but not after combined training. Reductions in diastolic BP (DBP) were observed after endurance (-2.5 mm Hg [-3.2 to -1.7]), dynamic resistance (-3.2 mm Hg [-4.5 to -2.0]), isometric resistance (-6.2 mm Hg [-10.3 to -2.0]), and combined (-2.2 mm Hg [-3.9 to -0.48]) training. BP reductions after endurance training were greater (P<0.0001) in 26 study groups of hypertensive subjects (-8.3 [-10.7 to -6.0]/-5.2 [-6.8 to -3.4] mm Hg) than in 50 groups of prehypertensive subjects (-2.1 [-3.3 to -0.83]/-1.7 [-2.7 to -0.68]) and 29 groups of subjects with normal BP levels (-0.75 [-2.2 to +0.69]/-1.1 [-2.2 to -0.068]). BP reductions after dynamic resistance training were largest for prehypertensive participants (-4.0 [-7.4 to -0.5]/-3.8 [-5.7 to -1.9] mm Hg) compared with patients with hypertension or normal BP.
Conclusion: Endurance, dynamic resistance, and isometric resistance training lower SBP and DBP, whereas combined training lowers only DBP. Data from a small number of isometric resistance training studies suggest this form of training has the potential for the largest reductions in SBP.
Figures
References
-
- Centers for Disease Control and Prevention Vital signs: prevalence, treatment, and control of hypertension—United States, 1999–2002 and 2005–2008. MMWR Morb Mortal Wkly Rep. 2011; 60:103-108 - PubMed
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors: 2001 systematic analysis of population health data. Lancet. 2006; 367:1747-1757 - PubMed
-
- Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD, Finkelstein EA, Hong Y, Johnston SC, Khera A, Lloyd‐Jones DM, Nelson SA, Nichol G, Orenstein D, Wilson PW, Woo YJAmerican Heart Association Advocacy Coordinating Committee, Stroke Council, Council on Cardiovascular Radiology and Intervention, Council on Clinical Cardiology, Council on Epidemiology and Prevention, Thrombosis and Vascular Biology, Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Cardiovascular Nursing, Council on the Kidney in Cardiovascular Disease, Council on Cardiovascular Surgery and Anesthesia, and Interdisciplinary Council on Quality of Care and Outcomes Research Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011; 123:933-944 - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, Roccella EJJoint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure. Hypertension. 2003; 42:1206-1252 - PubMed
-
- Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd‐Jones DM, Newby LK, Piña IL, Roger VL, Shaw LJ, Zhao D, Beckie TM, Bushnell C, D'Armiento J, Kris‐Etherton PM, Fang J, Ganiats TG, Gomes AS, Gracia CR, Haan CK, Jackson EA, Judelson DR, Kelepouris E, Lavie CJ, Moore A, Nussmeier NA, Ofili E, Oparil S, Ouyang P, Pinn VW, Sherif K, Smith SC, Jr, Sopko G, Chandra‐Strobos N, Urbina EM, Vaccarino V, Wenger NKAmerican Heart Association Effectiveness‐based guidelines for the prevention of cardiovascular disease in women–2011 update: a guideline from the American Heart Association. J Am Coll Cardiol. 2011; 57:1404-1423 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
