

A risk score for in-hospital death in patients admitted with ischemic or hemorrhagic stroke
- PMID: 23525444
- PMCID: PMC3603253
- DOI: 10.1161/JAHA.112.005207
A risk score for in-hospital death in patients admitted with ischemic or hemorrhagic stroke
Abstract
Background: We aimed to derive and validate a single risk score for predicting death from ischemic stroke (IS), intracerebral hemorrhage (ICH), and subarachnoid hemorrhage (SAH).
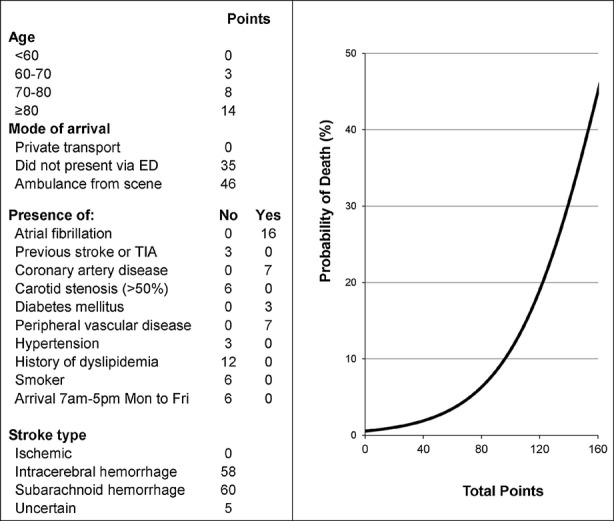
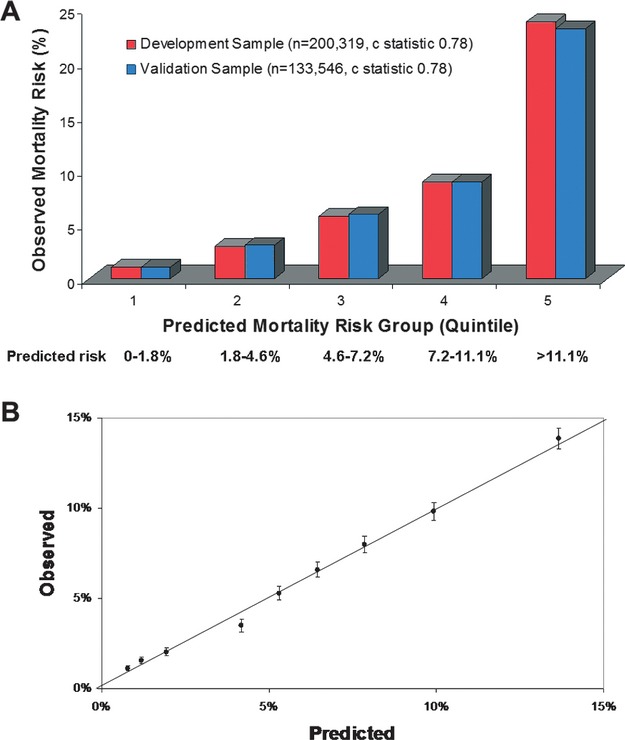
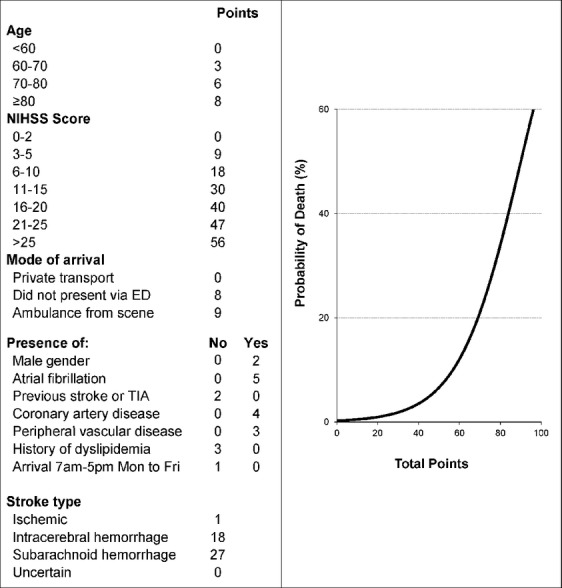
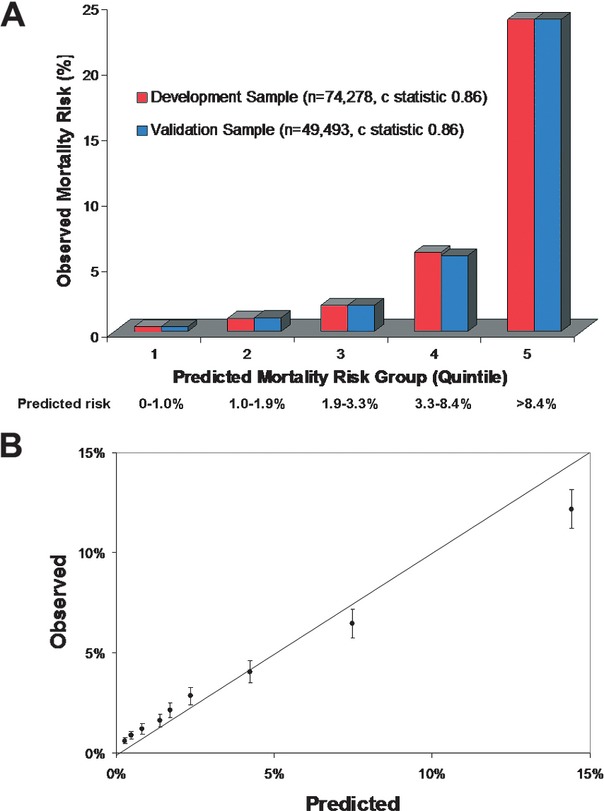
Methods and results: Data from 333 865 stroke patients (IS, 82.4%; ICH, 11.2%; SAH, 2.6%; uncertain type, 3.8%) in the Get With The Guidelines-Stroke database were used. In-hospital mortality varied greatly according to stroke type (IS, 5.5%; ICH, 27.2%; SAH, 25.1%; unknown type, 6.0%; P<0.001). The patients were randomly divided into derivation (60%) and validation (40%) samples. Logistic regression was used to determine the independent predictors of mortality and to assign point scores for a prediction model in the overall population and in the subset with the National Institutes of Health Stroke Scale (NIHSS) recorded (37.1%). The c statistic, a measure of how well the models discriminate the risk of death, was 0.78 in the overall validation sample and 0.86 in the model including NIHSS. The model with NIHSS performed nearly as well in each stroke type as in the overall model including all types (c statistics for IS alone, 0.85; for ICH alone, 0.83; for SAH alone, 0.83; uncertain type alone, 0.86). The calibration of the model was excellent, as demonstrated by plots of observed versus predicted mortality.
Conclusions: A single prediction score for all stroke types can be used to predict risk of in-hospital death following stroke admission. Incorporation of NIHSS information substantially improves this predictive accuracy.
Figures
References
-
- Counsell C, Dennis M, McDowall M, Warlow C. Predicting outcome after acute and subacute stroke: development and validation of new prognostic models. Stroke. 2002; 33:1041-1047 - PubMed
-
- Johnston KC, Wagner DP, Wang XQ, Newman GC, Thijs V, Sen S, Warach S. Validation of an acute ischemic stroke model: does diffusion‐weighted imaging lesion volume offer a clinically significant improvement in prediction of outcome? Stroke. 2007; 38:1820-1825 - PubMed
-
- Weimar C, Ziegler A, Konig IR, Diener HC. Predicting functional outcome and survival after acute ischemic stroke. J Neurol. 2002; 249:888-895 - PubMed
-
- Weimar C, Konig IR, Kraywinkel K, Ziegler A, Diener HC. Age and National Institutes of Health Stroke Scale Score within 6 hours after onset are accurate predictors of outcome after cerebral ischemia: development and external validation of prognostic models. Stroke. 2004; 35:158-162 - PubMed
-
- Hinchey JA, Furlan AJ, Frank JI, Kay R, Misch D, Hill C. Is in‐hospital stroke mortality an accurate measure of quality of care? Neurology. 1998; 50:619-625 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
