

A 22-year Northern Irish experience of carotid body tumours
- PMID: 23526121
- PMCID: PMC3605524
A 22-year Northern Irish experience of carotid body tumours
Abstract
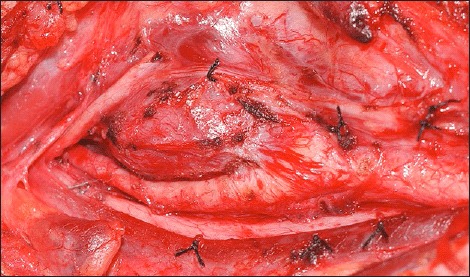
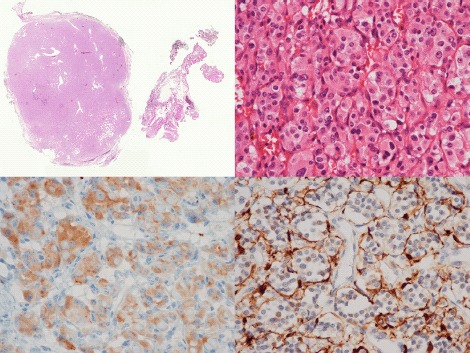
Objectives: Carotid body tumours (CBTs) are rare vascular neoplasms originating in paraganglionic cells of the carotid bifurcation. The aim of this study was to review all patients diagnosed with CBTs in Northern Ireland.
Methods: A retrospective review was performed of all patients who had CBTs treated at our institutions between 1987 and 2009. Patient demographics, clinical symptomatology, investigative modality, therapeutic intervention, pathological analysis and long-term outcomes were assessed.
Results: Twenty-nine patients were identified with 33 CBTs and three glomus intravagale tumours (GITs). Six patients had bilateral CBTs (21%), one of whom had a synchronous GIT. Twenty-six patients underwent a total of 30 operative procedures for the resection of 28 CBTs and 3 GITs. Conventional operative treatment included subadventitial tumour excision. A vascular shunt facilitated arterial reconstruction following the removal of seven (23%) tumours and on six of these occasions (19%) continuity was restored with an interposition vein graft. For access the external carotid artery was ligated during the removal of four tumours (13%). Two tumours were considered malignant. No peri-operative mortalities were recorded. Immediate complications included peri-operative stroke secondary to an occluded vein graft (n=1), requirement of tracheostomy (n=2), emergency haematoma drainage (n=2) and transient cranial nerve damage (n=8). Late complications included pseudoaneurysm of vein graft with subsequent stoke (n=1), permanent cranial nerve damage (n=9), Horner's syndrome (n=1) and an asymptomatic vein graft occlusion (n=1). One patient had tumour recurrence two years post-operatively and died due to pulmonary metastases. Two other patients died of unrelated causes. All other patients remain well with no evidence of tumour recurrence at mean followup of 1801 days (range 159-9208 days).
Conclusion: Our long-term experience is comparable with other reported case series where surgical intervention conferred a long-term survival advantage despite associated cranial nerve co-morbidities.
Keywords: Carotid Body; Complications; Outcome; Surgery; Tumour.
Figures



References
-
- Sajid MS, Hamilton G, Baker DM. A multicentre review of carotid body tumour management. Eur J Vasc Endovasc Surg. 2007;34(2):127–30. - PubMed
-
- Plukker JT, Brongers EP, Vermey A, Krikke A, van den Dungen JJ. Outcome of surgical treatment for carotid body paraganglioma. Br J Surg. 2001;88(10):1382–6. - PubMed
-
- Rodriguez-Cuevas S., Lopez-Garza J, Labastidia-Almendaro S. Carotid body tumors in inhabitants of altitudes higher than 2000 meters above sea level. Head Neck. 1998;20(5):374–8. - PubMed
-
- Luna-Ortiz K, Rascon-Ortiz M, Villavicencio-Valencia V, Granados-Garcia M, Herrera-Gomez A. Carotid body tumours: a review of a 20 year experience. Oral Oncol. 2005;41(1):56–61. - PubMed
-
- Wang SJ, Wang MB, Barauskas TM, Calcaterra TC. Surgical management of carotid body tumors. Otolaryngol Head Neck Surg. 2000;123(3):202–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources