

Effects of population based screening for Chlamydia infections in the Netherlands limited by declining participation rates
- PMID: 23527005
- PMCID: PMC3604006
- DOI: 10.1371/journal.pone.0058674
Effects of population based screening for Chlamydia infections in the Netherlands limited by declining participation rates
Abstract
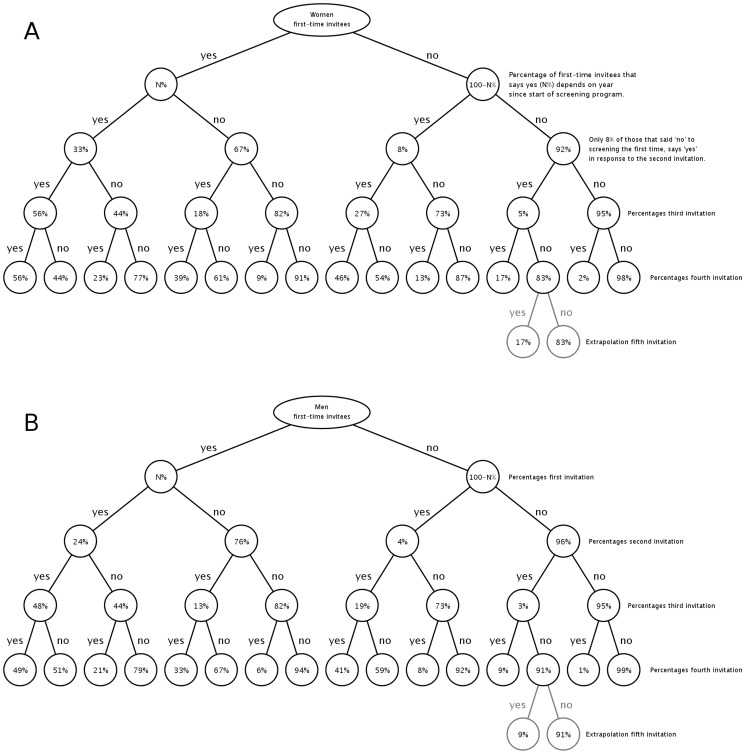
Background: A large trial to investigate the effectiveness of population based screening for chlamydia infections was conducted in the Netherlands in 2008-2012. The trial was register based and consisted of four rounds of screening of women and men in the age groups 16-29 years in three regions in the Netherlands. Data were collected on participation rates and positivity rates per round. A modeling study was conducted to project screening effects for various screening strategies into the future.
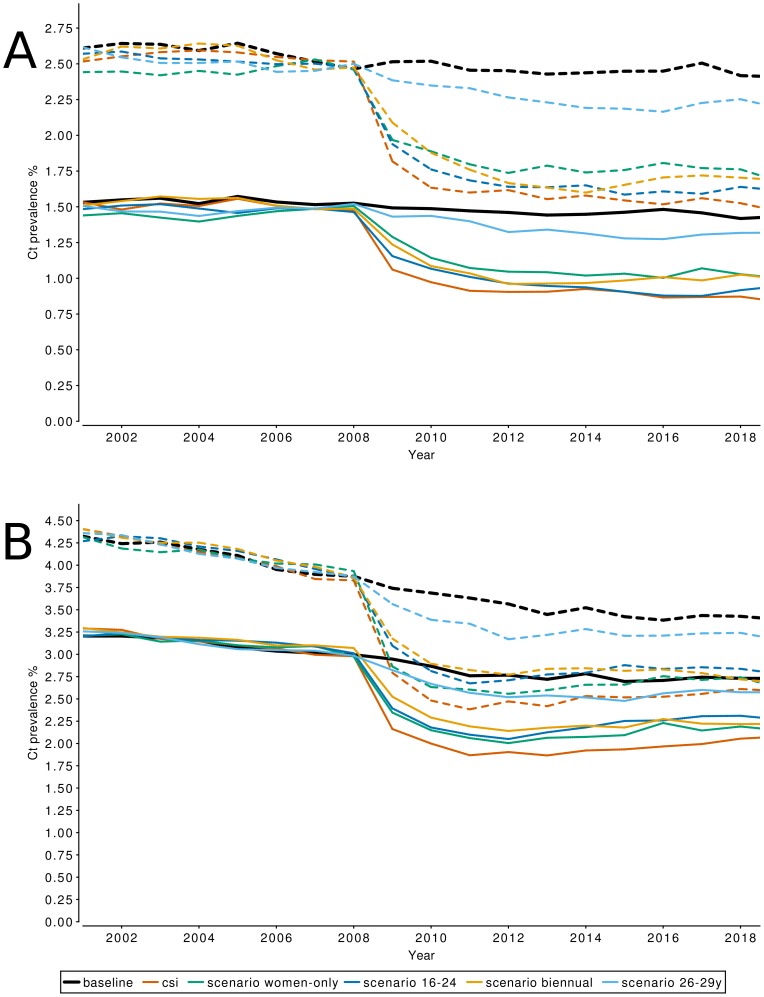
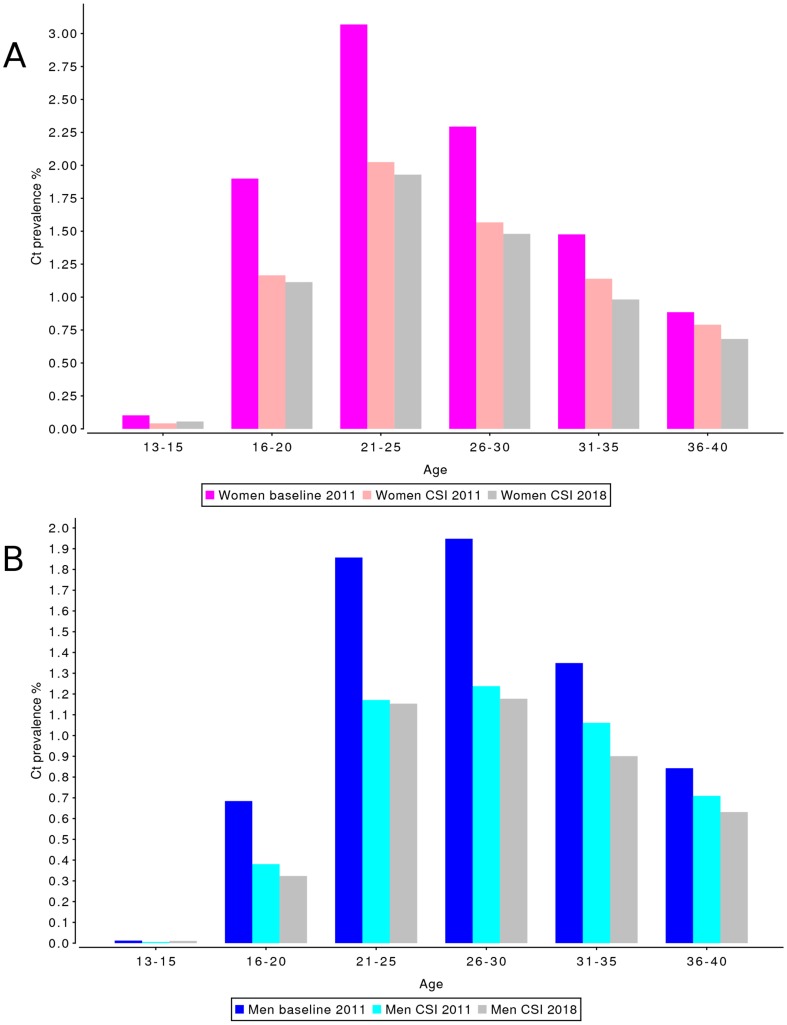
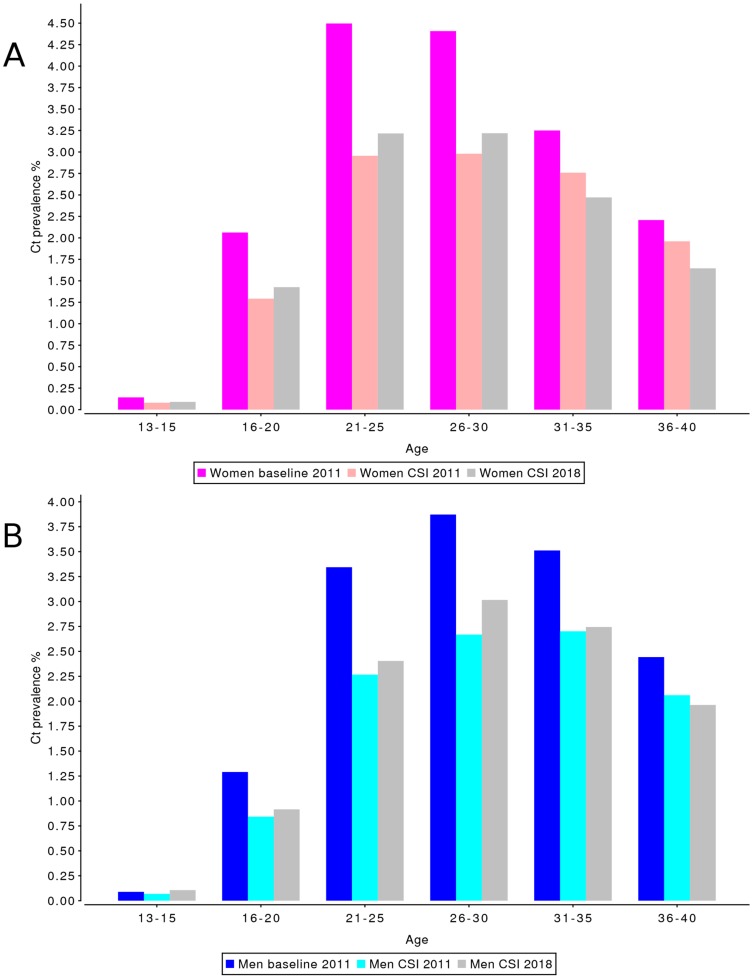
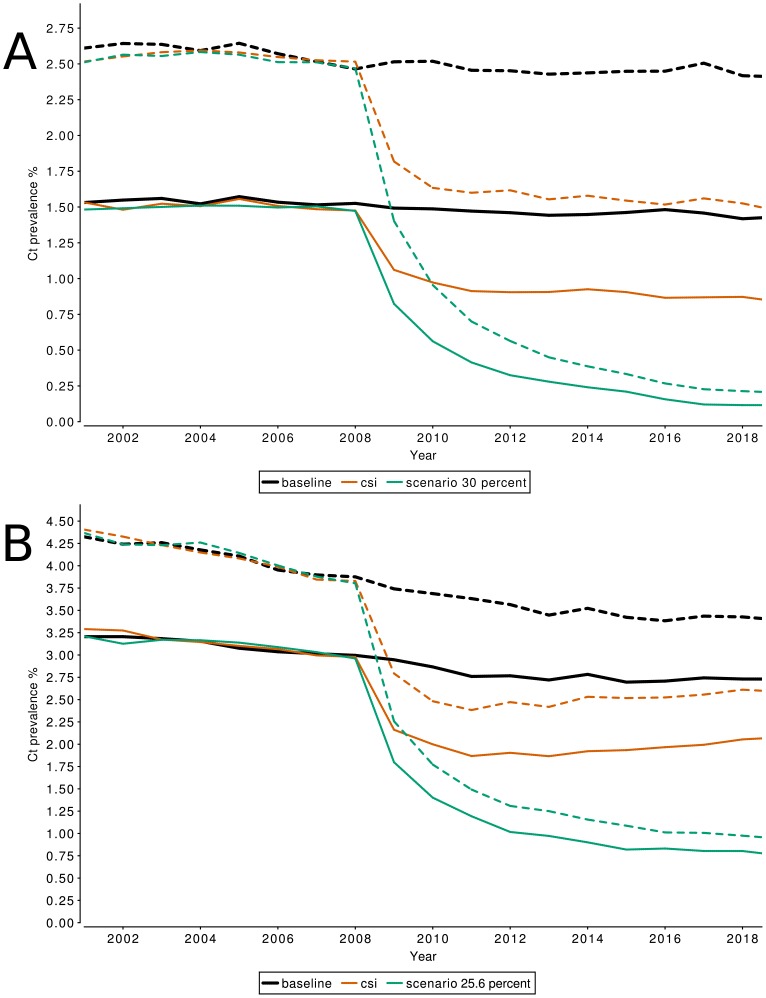
Methods and findings: We used a stochastic network simulation model incorporating partnership formation and dissolution, aging and a sexual life course perspective. Trends in baseline rates of chlamydia testing and treatment were used to describe the epidemiological situation before the start of the screening program. Data on participation rates was used to describe screening uptake in rural and urban areas. Simulations were used to project the effectiveness of screening on chlamydia prevalence for a time period of 10 years. In addition, we tested alternative screening strategies, such as including only women, targeting different age groups, and biennial screening. Screening reduced prevalence by about 1% in the first two screening rounds and leveled off after that. Extrapolating observed participation rates into the future indicated very low participation in the long run. Alternative strategies only marginally changed the effectiveness of screening. Higher participation rates as originally foreseen in the program would have succeeded in reducing chlamydia prevalence to very low levels in the long run.
Conclusions: Decreasing participation rates over time profoundly impact the effectiveness of population based screening for chlamydia infections. Using data from several consecutive rounds of screening in a simulation model enabled us to assess the future effectiveness of screening on prevalence. If participation rates cannot be kept at a sufficient level, the effectiveness of screening on prevalence will remain limited.
Conflict of interest statement
Figures
References
-
- van Bergen J, Gotz HM, Richardus JH, Hoebe CJ, Broer J, et al. (2005) Prevalence of urogenital Chlamydia trachomatis increases significantly with level of urbanisation and suggests targeted screening approaches: results from the first national population based study in the Netherlands. Sex Transm Infect 81: 17–23. - PMC - PubMed
-
- van Bergen JE, Spaargaren J, Gotz HM, Veldhuijzen IK, Bindels PJ, et al. (2006) Population prevalence of Chlamydia trachomatis and Neisseria gonorrhoeae in the Netherlands. Should asymptomatic persons be tested during population-based Chlamydia screening also for gonorrhoea or only if chlamydial infection is found? BMC Infect Dis 6: 42. - PMC - PubMed
-
- Land JA, Van Bergen JE, Morre SA, Postma MJ (2010) Epidemiology of Chlamydia trachomatis infection in women and the cost-effectiveness of screening. Hum Reprod Update 16: 189–204. - PubMed
-
- Johnson RE, Berman S (2010) Sexual Transmission: Chlamydia trachomatis. In: Krämer A, Kretzschmar M, Krickeberg K, editors. Modern Infectious Disease Epidemiology: Concepts, Methods, Mathematical Models, and Public Health. New York: Springer Verlag.pp. 359–382.
-
- Health Council of the Netherlands (2004) Screening for Chlamydia. The Hague: Health Council of the Netherlands.2004/07 2004/07.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
