

Early phase trial design for assessing several dose levels for toxicity and efficacy for targeted agents
- PMID: 23529697
- PMCID: PMC3744092
- DOI: 10.1177/1740774513480961
Early phase trial design for assessing several dose levels for toxicity and efficacy for targeted agents
Abstract
Background: Traditional phase I trials are designed to be conservative. Many times a traditional phase I trial design stops at a dose level below the maximal tolerated dose (MTD), thus potentially treating patients at a suboptimal level in all subsequent trials. This has been confirmed by our recent simulation studies.
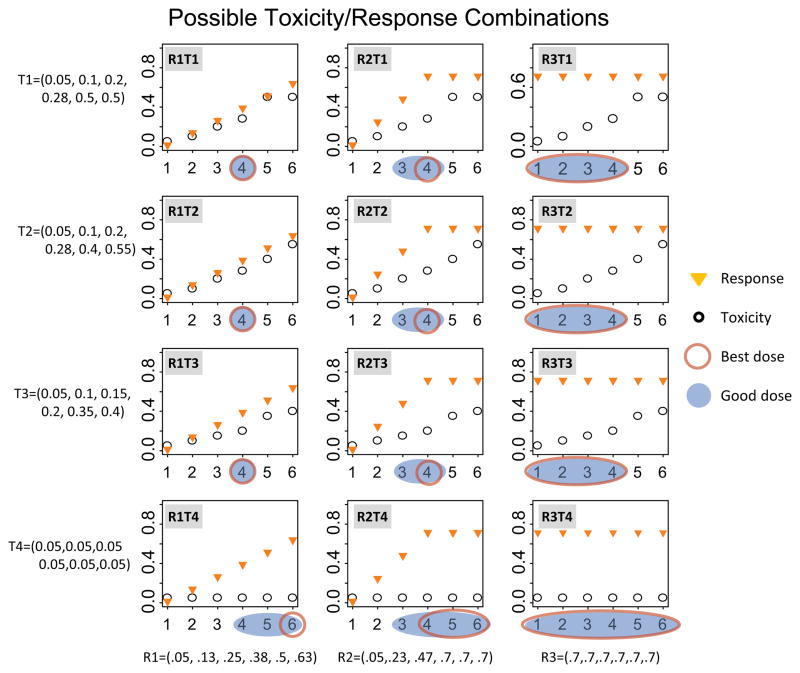
Purpose: We propose a phase I/II trial design to determine the most promising dose level in terms of toxicity and efficacy for cytostatic or targeted agents. This design evaluates three dose levels for efficacy and toxicity using a modified phase II selection design. The dose levels include the phase I recommended dose (RD) in addition to the dose levels immediately below and above that level.
Methods: This phase I/II trial design uses a two-step approach. In the first step, a traditional phase I trial design is used to get close to a good dose level. The second step consists of a modified selection design, randomizing patients to three dose levels: the phase I RD level and the dose levels immediately below and above the phase I RD level. Both efficacy and toxicity are used to determine a good or best dose level. Appropriate toxicity stopping rules in the phase II portion of the trial are implemented as part of such a trial. We perform simulation studies for a variety of toxicity and efficacy scenarios to determine the operating characteristics of this design and compare those to our originally proposed trial where we only explore dose levels at and below the phase I RD in the second phase of the trial, as well as to the traditional setting where a phase I trial is followed by a single-arm phase II trial at the phase I RD.
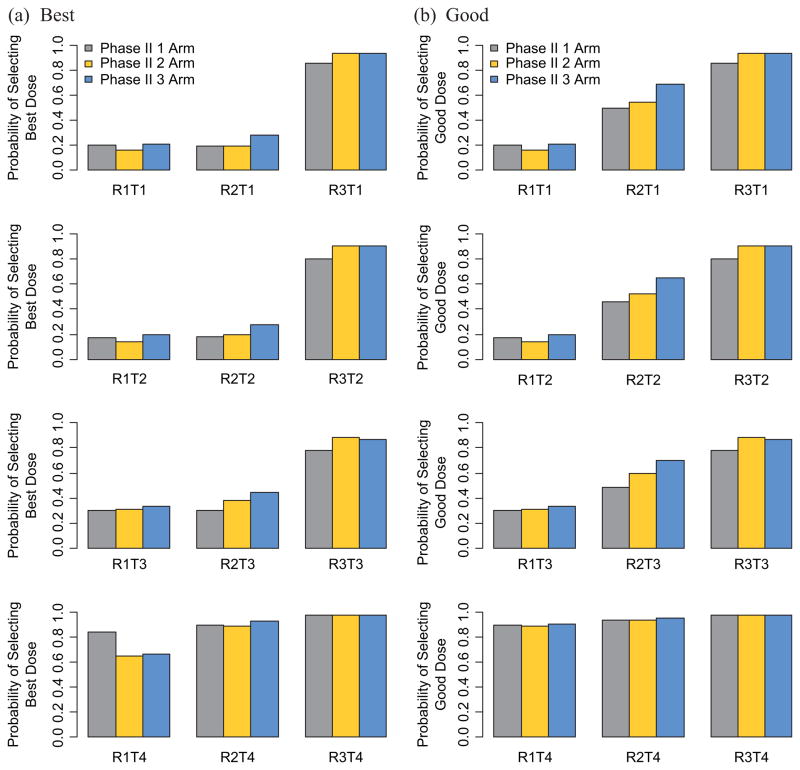
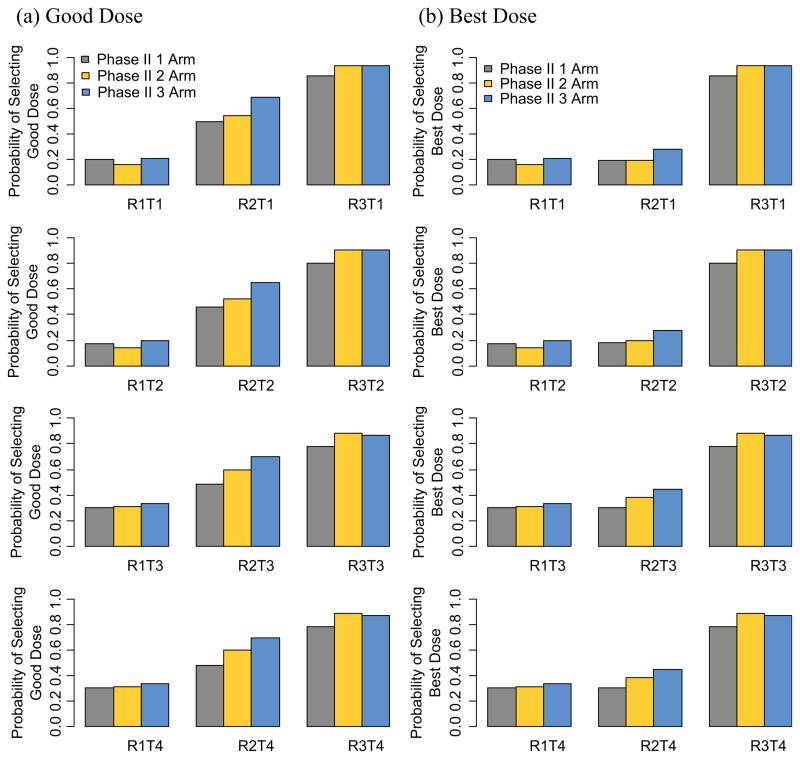
Results: The 3-arm modified selection design exploring the dose levels immediately above and below as well as the RD performs as well or better than the 2-arm modified selection design or the single-arm design for almost all toxicity and efficacy scenario combinations tested.
Conclusion: We demonstrate that this design has a higher success rate at identifying a good or best dose level when exploring dose levels immediately above and below the RD in the early phase II setting, in most cases without needing larger sample sizes.
Conflict of interest statement
None declared.
Figures
References
-
- Hoering A, LeBlanc M, Crowley J. Seamless phase I/II trial design for assessing toxicity and efficacy for targeted agents. In: Crowley J, Hoering A, editors. Handbook of Statistics in Clinical Oncology. 3. Boca Raton, London, New York: CRC Press; 2012. pp. 97–106.
-
- Storer BE. Choosing a phase I design. In: Crowley J, Hoering A, editors. Handbook of Statistics in Clinical Oncology. 3. Boca Raton, London, New York: CRC Press; 2012. pp. 85–95.
-
- Penel N, Isambert N, Leblond P, et al. ‘Classical 3 + 3 design’ versus ‘accelerated titration designs’: Analysis of 270 phase I trials investigating anti-cancer agents. Invest New Drugs. 2009;27:552–56. - PubMed
-
- Ivy P, Siu L, Garrett-Mayer E. Approaches to phase I clinical trial design focused on safety, efficiency and selected patient populations: A report from the clinical trial design task force of the National Cancer Institute investigational drug steering committee. Clin Cancer Res. 2010;16:1726–36. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
