

Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient--2013 update: cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery
- PMID: 23529939
- PMCID: PMC4142593
- DOI: 10.1002/oby.20461
Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient--2013 update: cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery
Abstract
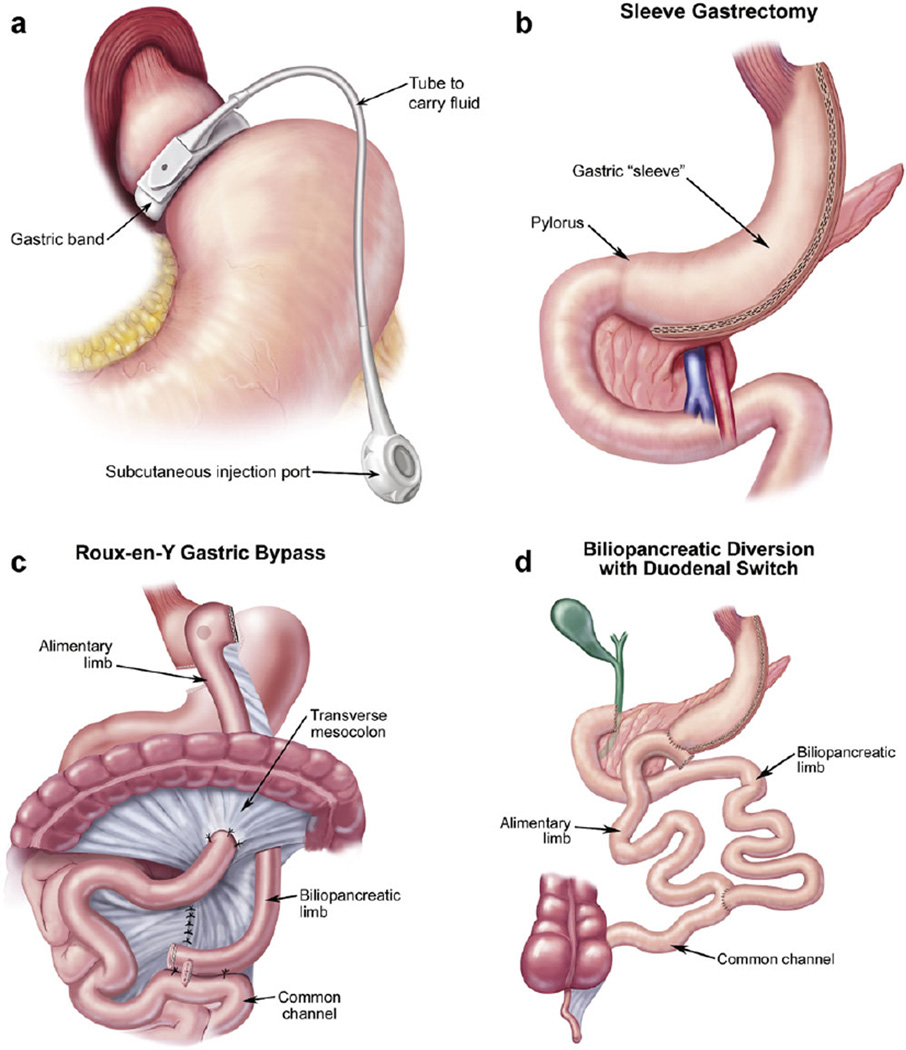
The development of these updated guidelines was commissioned by the AACE, TOS, and ASMBS Board of Directors and adheres to the AACE 2010 protocol for standardized production of clinical practice guidelines (CPG). Each recommendation was re-evaluated and updated based on the evidence and subjective factors per protocol. Examples of expanded topics in this update include: the roles of sleeve gastrectomy, bariatric surgery in patients with type-2 diabetes, bariatric surgery for patients with mild obesity, copper deficiency, informed consent, and behavioral issues. There are 74 recommendations (of which 56 are revised and 2 are new) in this 2013 update, compared with 164 original recommendations in 2008. There are 403 citations, of which 33 (8.2%) are EL 1, 131 (32.5%) are EL 2, 170 (42.2%) are EL 3, and 69 (17.1%) are EL 4. There is a relatively high proportion (40.4%) of strong (EL 1 and 2) studies, compared with only 16.5% in the 2008 AACE-TOS-ASMBS CPG. These updated guidelines reflect recent additions to the evidence base. Bariatric surgery remains a safe and effective intervention for select patients with obesity. A team approach to perioperative care is mandatory with special attention to nutritional and metabolic issues.
Copyright © 2013 The Obesity Society.
Conflict of interest statement
Jeffrey I. Mechanick, M.D.: Abbott Nutrition, honoraria for lectures and program development. Daniel B. Jones, M.D., M.S.: Allurion, consultant. W. Timothy Garvey, M.D.: Merck, speakers list; Daiichi-Sanyo, Vivus, Alkermes, Liposcience, Tethys Bioscience, advisory boards; Merck, Amylin, Weight Watchers, research. Scott Shikora, M.D.: Baxter Healthcare, consultant; EnteroMedics, consultant; GI Dynamics, stock options for previous consultant work. John B. Dixon, M.B.B.S., Ph.D.: Consultant for Allergan Inc. and Bariatric Advantage Inc.; Scientific Advisory Board for OPTIFAST(R), Nestle Australia; developed educational material and is on the speakers’ bureau for iNova Pharmaceuticals; Institutions receive research assistance from Allergan Inc. and Nestle Australia. Robin Blackstone, M.D.: Enteromedics PI and Johnson and Johnson, consultant. Alan Garber, M.D.: Novo Nordisk, Daiichi Sankyo, Merck, Takeda, Santarus, LipoScience, Boehringer Ingelheim, Tethys, Lexicon, Vivus, consultant; Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, advisory board; Merck, Novo Nordisk, Santarus, Daiichi Sankyo, Speakers Bureau. Stacy Brethauer, M.D.: Ethicon Endo-Surgery, consultant and Advisory Board member. David B. Sarwer, Ph.D.: Allergan, BaroNova, EnteroMedics, Ethicon Endo- Surgery, Galderma, consultant. Bruce Wolfe, M.D.: EnteroMedics, investigator. Adrienne Youdim, M.D., Daniel L. Hurley, M.D., M. Molly McMahon, M.D., Leslie J. Heinberg, Ph.D., Robert Kushner, M.D., Ted Adams, Ph.D., M.P.H., George Blackburn, M.D., Ph.D., and Christopher D. Still, D.O., report no potential conflicts of interest.
Figures
References
-
- Ogden CL, Carroll MD, Kit BK, et al. Prevalence of obesity in the United States, 20092013;2020. NCHS Data Brief. 2012;82:1–8. EL, SS. - PubMed
-
- Mechanick JI, Garber AJ, Handelsman Y, et al. American Association of Clinical Endocrinologists (AACE) position paper on obesity and obesity medicine. Endocr Pract. 2012;18:642–648. EL 4, NE position. - PubMed
-
- Ryan DH, Johnson WD, Myers VH, et al. Nonsurgical weight loss for extreme obesity in primary care settings: results of the Louisiana Obese Subjects Study. Arch Intern Med. 2010;170:146–154. EL 1, RCT. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
