

Impact of diuretic therapy-associated electrolyte disorders present on admission to the emergency department: a cross-sectional analysis
- PMID: 23531202
- PMCID: PMC3621479
- DOI: 10.1186/1741-7015-11-83
Impact of diuretic therapy-associated electrolyte disorders present on admission to the emergency department: a cross-sectional analysis
Abstract
Background: Diuretics are among the most commonly prescribed medications and, due to their mechanisms of action, electrolyte disorders are common side effects of their use. In the present work we investigated the associations between diuretics being taken and the prevalence of electrolyte disorders on admission as well as the impact of electrolyte disorders on patient outcome.
Methods: In this cross sectional analysis, all patients presenting between 1 January 2010 and 31 December 2011 to the emergency room (ER) of the Inselspital, University Hospital Bern, Switzerland were included. Data on diuretic medication, baseline characteristics and laboratory data including electrolytes and renal function parameters were obtained from all patients. A multivariable logistic regression model was performed to assess the impact of factors on electrolyte disorders and patient outcome.
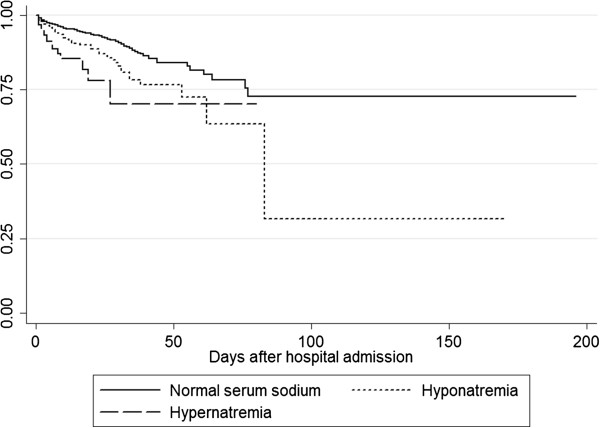
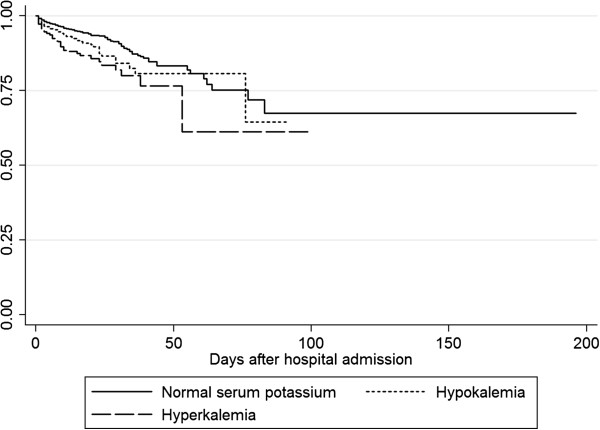
Results: A total of 8.5% of patients presenting to the ER used one diuretic, 2.5% two, and 0.4% three or four. In all, 4% had hyponatremia on admission and 12% hypernatremia. Hypokalemia was present in 11% and hyperkalemia in 4%. All forms of dysnatremia and dyskalemia were more common in patients taking diuretics. Loop diuretics were an independent risk factor for hypernatremia and hypokalemia, while thiazide diuretics were associated with the presence of hyponatremia and hypokalemia. In the Cox regression model, all forms of dysnatremia and dyskalemia were independent risk factors for in hospital mortality.
Conclusions: Existing diuretic treatment on admission to the ER was associated with an increased prevalence of electrolyte disorders. Diuretic therapy itself and disorders of serum sodium and potassium were risk factors for an adverse outcome.
Figures
References
-
- Rose BD, Post TW. Clinical Physiology of Acid–base and Electrolyte Disorders. Volume 15 5. New York, NY: McGraw Hill; 2001. Clinical use of diuretics.
-
- Gross P, Palm C. Thiazides: do they kill? Nephrol Dial Transplant. 2005;20:2299–2301. - PubMed
-
- Siegel D, Hulley SB, Black DM, Cheitlin MD, Sebastian A, Seeley DG, Hearst N, Fine R. Diuretics, serum and intracellular electrolyte levels, and ventricular arrhythmias in hypertensive men. JAMA. 1992;267:1083–1089. - PubMed
-
- Leung AA, Wright A, Pazo V, Karson A, Bates DW. Risk of thiazide-induced hyponatremia in patients with hypertension. Am J Med. 2011;124:1064–1072. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
