

Effect of disodium EDTA chelation regimen on cardiovascular events in patients with previous myocardial infarction: the TACT randomized trial
- PMID: 23532240
- PMCID: PMC4066975
- DOI: 10.1001/jama.2013.2107
Effect of disodium EDTA chelation regimen on cardiovascular events in patients with previous myocardial infarction: the TACT randomized trial
Abstract
Importance: Chelation therapy with disodium EDTA has been used for more than 50 years to treat atherosclerosis without proof of efficacy.
Objective: To determine if an EDTA-based chelation regimen reduces cardiovascular events.
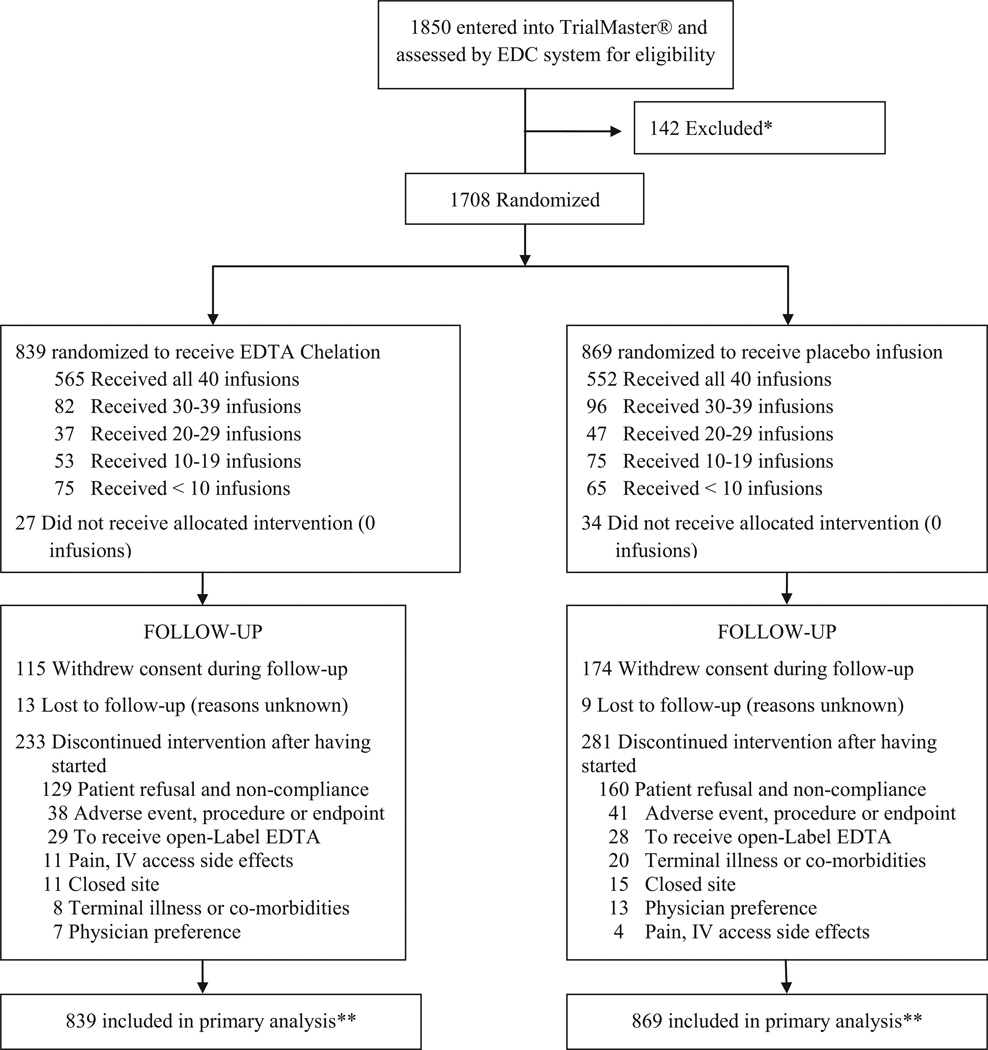
Design, setting, and participants: Double-blind, placebo-controlled, 2 × 2 factorial randomized trial enrolling 1708 patients aged 50 years or older who had experienced a myocardial infarction (MI) at least 6 weeks prior and had serum creatinine levels of 2.0 mg/dL or less. Participants were recruited at 134 US and Canadian sites. Enrollment began in September 2003 and follow-up took place until October 2011 (median, 55 months). Two hundred eighty-nine patients (17% of total; n=115 in the EDTA group and n=174 in the placebo group) withdrew consent during the trial.
Interventions: Patients were randomized to receive 40 infusions of a 500-mL chelation solution (3 g of disodium EDTA, 7 g of ascorbate, B vitamins, electrolytes, procaine, and heparin) (n=839) vs placebo (n=869) and an oral vitamin-mineral regimen vs an oral placebo. Infusions were administered weekly for 30 weeks, followed by 10 infusions 2 to 8 weeks apart. Fifteen percent discontinued infusions (n=38 [16%] in the chelation group and n=41 [15%] in the placebo group) because of adverse events.
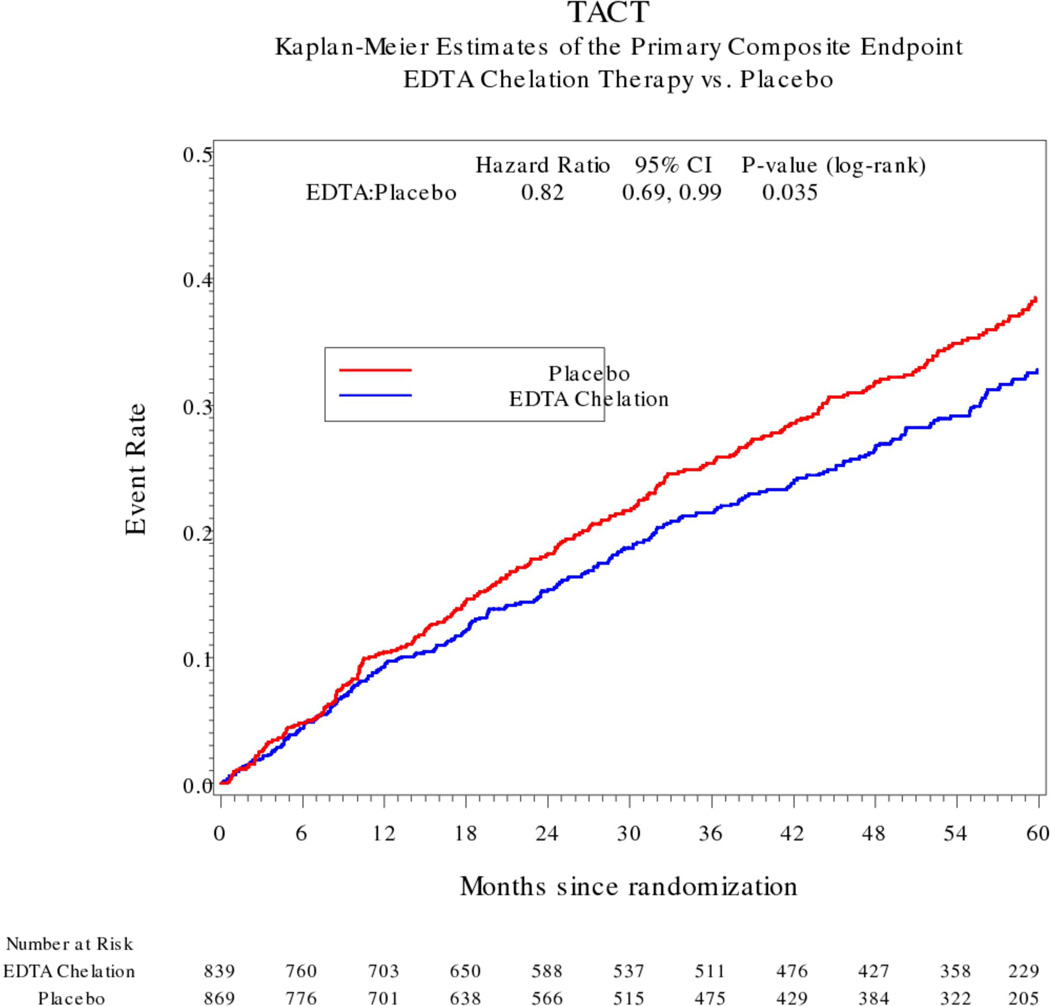
Main outcome measures: The prespecified primary end point was a composite of total mortality, recurrent MI, stroke, coronary revascularization, or hospitalization for angina. This report describes the intention-to-treat comparison of EDTA chelation vs placebo. To account for multiple interim analyses, the significance threshold required at the final analysis was P = .036.
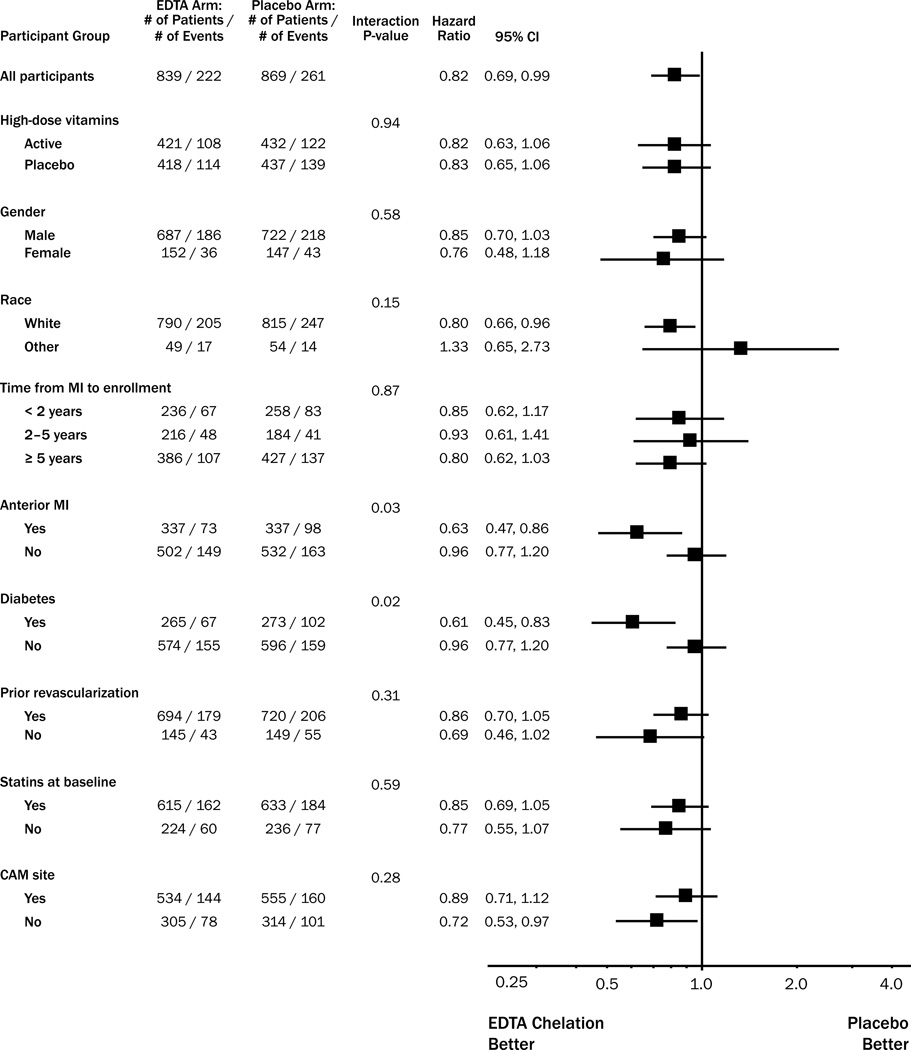
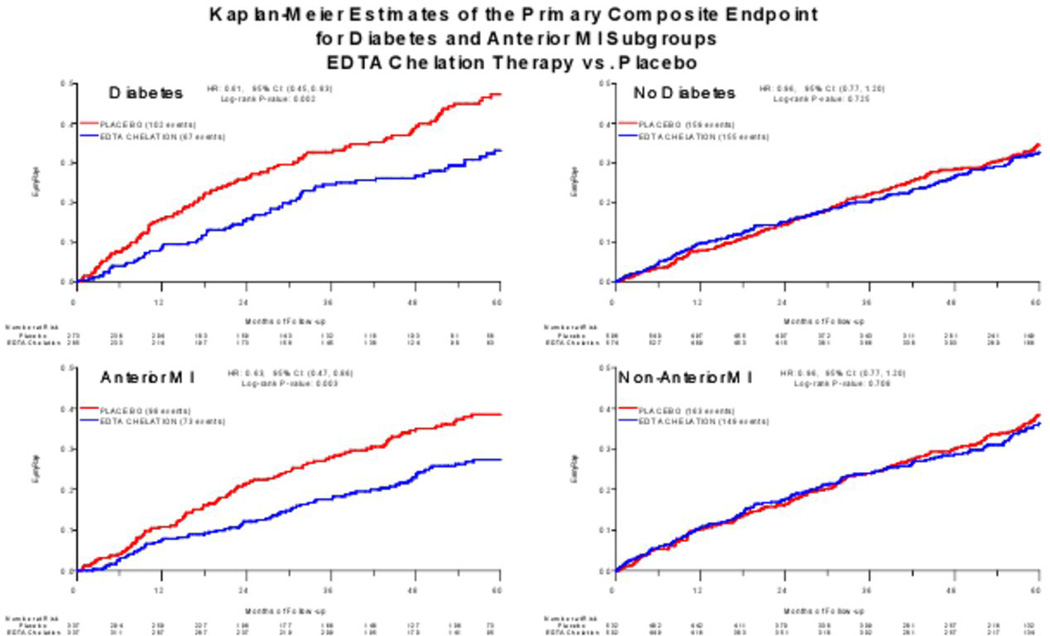
Results: Qualifying previous MIs occurred a median of 4.6 years before enrollment. Median age was 65 years, 18% were female, 9% were nonwhite, and 31% were diabetic. The primary end point occurred in 222 (26%) of the chelation group and 261 (30%) of the placebo group (hazard ratio [HR], 0.82 [95% CI, 0.69-0.99]; P = .035). There was no effect on total mortality (chelation: 87 deaths [10%]; placebo, 93 deaths [11%]; HR, 0.93 [95% CI, 0.70-1.25]; P = .64), but the study was not powered for this comparison. The effect of EDTA chelation on the components of the primary end point other than death was of similar magnitude as its overall effect (MI: chelation, 6%; placebo, 8%; HR, 0.77 [95% CI, 0.54-1.11]; stroke: chelation, 1.2%; placebo, 1.5%; HR, 0.77 [95% CI, 0.34-1.76]; coronary revascularization: chelation, 15%; placebo, 18%; HR, 0.81 [95% CI, 0.64-1.02]; hospitalization for angina: chelation, 1.6%; placebo, 2.1%; HR, 0.72 [95% CI, 0.35-1.47]). Sensitivity analyses examining the effect of patient dropout and treatment adherence did not alter the results.
Conclusions and relevance: Among stable patients with a history of MI, use of an intravenous chelation regimen with disodium EDTA, compared with placebo, modestly reduced the risk of adverse cardiovascular outcomes, many of which were revascularization procedures. These results provide evidence to guide further research but are not sufficient to support the routine use of chelation therapy for treatment of patients who have had an MI.
Trial registration: clinicaltrials.gov Identifier: NCT00044213.
Figures
Comment in
-
Evaluation of the Trial to Assess Chelation Therapy (TACT): the scientific process, peer review, and editorial scrutiny.JAMA. 2013 Mar 27;309(12):1291-2. doi: 10.1001/jama.2013.2761. JAMA. 2013. PMID: 23532245 No abstract available.
-
Concerns about reliability in the Trial to Assess Chelation Therapy (TACT).JAMA. 2013 Mar 27;309(12):1293-4. doi: 10.1001/jama.2013.2778. JAMA. 2013. PMID: 23532246 No abstract available.
-
Chelation therapy and cardiovascular outcomes.JAMA. 2013 Jul 24;310(4):430-1. doi: 10.1001/jama.2013.7933. JAMA. 2013. PMID: 23917297 No abstract available.
-
Chelation therapy and cardiovascular outcomes.JAMA. 2013 Jul 24;310(4):431. doi: 10.1001/jama.2013.7930. JAMA. 2013. PMID: 23917299 No abstract available.
-
Chelation therapy and cardiovascular outcomes--in reply.JAMA. 2013 Jul 24;310(4):431-2. doi: 10.1001/jama.2013.7954. JAMA. 2013. PMID: 23917300 No abstract available.
References
-
- Bessman SP, Ried H, Rubin M. Treatment of lead encephalopathy with calcium disodium versenate. Med Ann DC. 1952;31:312–314. - PubMed
-
- Clarke NE, Clarke CN, Mosher RE. The in vivo dissolution of metastatic calcium; an approach to atherosclerosis. Am J Med Sci. 1955;229(2):142–149. - PubMed
-
- Clarke NE, Clarke CN, Mosher RE. Treatment of angina pectoris with disodium ethylene diamine tetraacetic acid. Am J Med Sci. 1956;232(6):654–666. - PubMed
-
- Casdorph HR. EDTA chelation therapy - efficacy in arteriosclerotic heart disease. J Holistic Med. 1981;3:53.
-
- Grier MT, Meyers DG. So much writing, so little science: A review of 37 years of literature on Edetate Sodium chelation therapy. Ann Pharmacother. 1993;27:1504–1509. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
