

Expression of calcineurin activity after lung transplantation: a 2-year follow-up
- PMID: 23536885
- PMCID: PMC3607585
- DOI: 10.1371/journal.pone.0059634
Expression of calcineurin activity after lung transplantation: a 2-year follow-up
Abstract
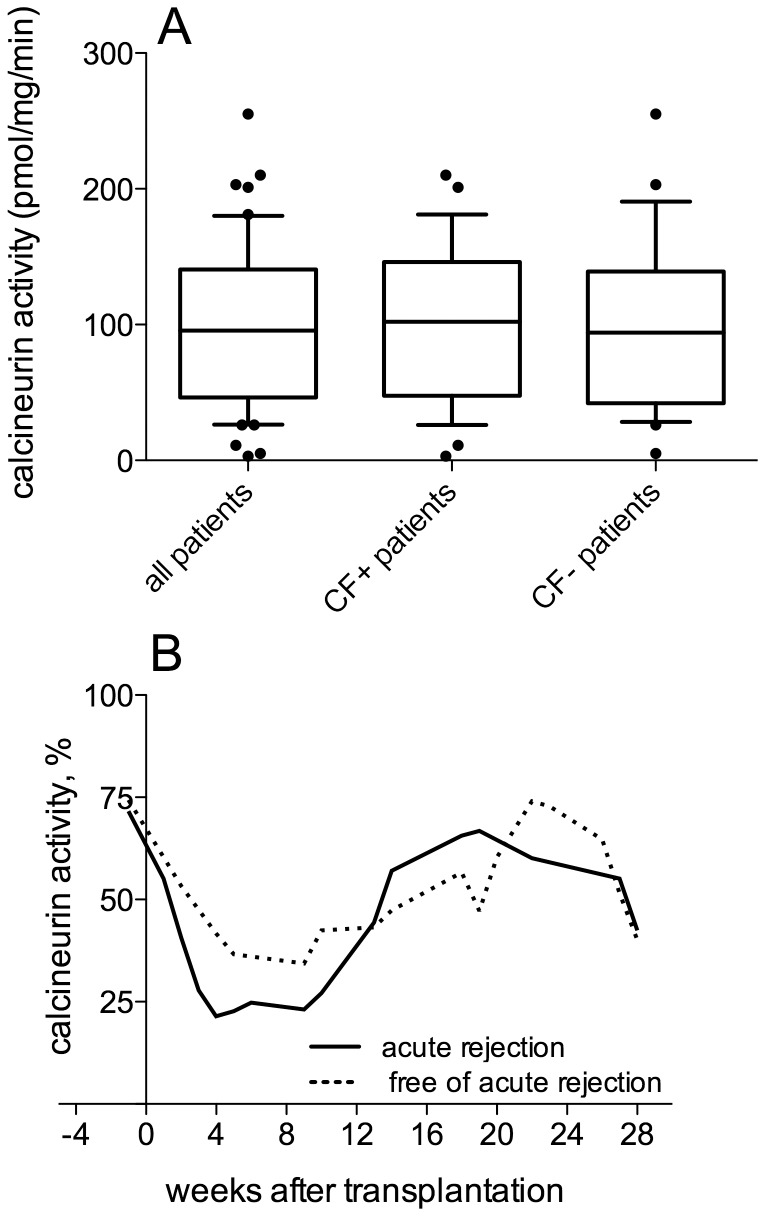
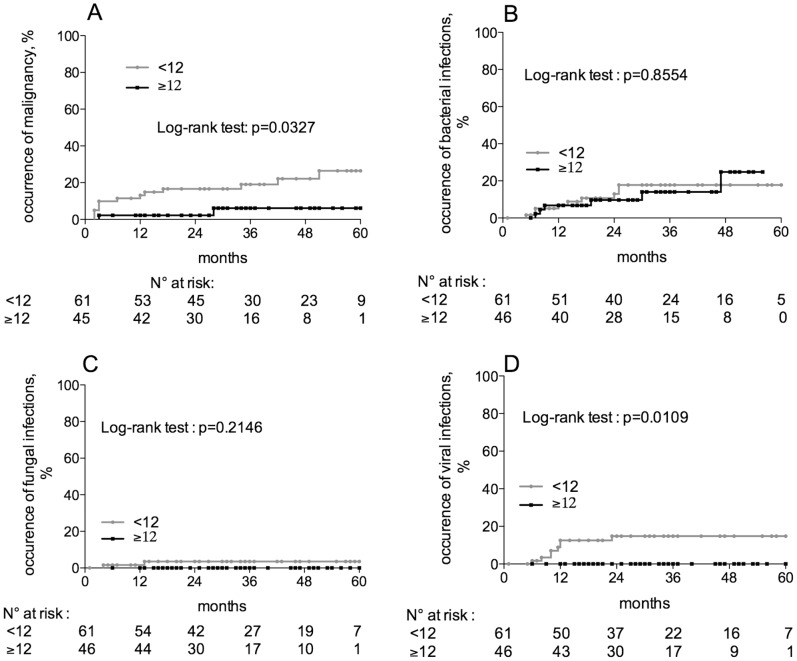
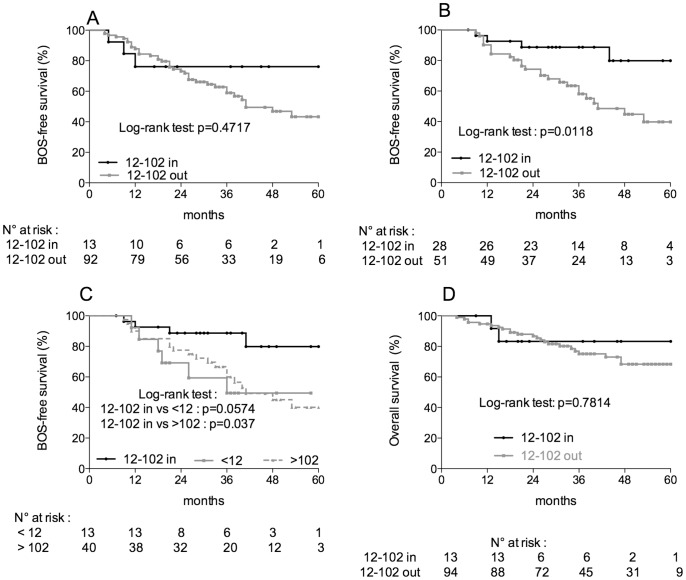
The objective of this pharmacodynamic study was to longitudinally assess the activity of calcineurin during the first 2 years after lung transplantation. From March 2004 to October 2008, 107 patients were prospectively enrolled and their follow-up was performed until 2009. Calcineurin activity was measured in peripheral blood mononuclear cells. We report that calcineurin activity was linked to both acute and chronic rejection. An optimal activity for calcineurin with two thresholds was defined, and we found that the risk of rejection was higher when the enzyme activity was above the upper threshold of 102 pmol/mg/min or below the lower threshold of 12 pmol/mg/min. In addition, we report that the occurrence of malignancies and viral infections was significantly higher in patients displaying very low levels of calcineurin activity. Taken together, these findings suggest that the measurement of calcineurin activity may provide useful information for the management of the prevention therapy of patients receiving lung transplantation.
Conflict of interest statement
Figures
References
-
- American Thoracic Society (1998) International guidelines for the selection of lung transplant candidates. Am J Respir Crit Care Med 158: 335–339. - PubMed
-
- Lin HM, Kauffman HM, McBride MA, Davies DB, Rosendale JD, et al. (1998) Center-specific graft and patient survival rates: 1997 United Network for Organ Sharing (UNOS) report. JAMA 280: 1153–1160. - PubMed
-
- Bando K, Paradis IL, Similo S, Konishi H, Komatsu K, et al. (1995) Obliterative bronchiolitis after lung and heart-lung transplantation: an analysis of risk factors and management. J Thorac Cardiovasc Surg 110: 4–13. - PubMed
-
- Sharples LD, Tamm M, McNeil K, Higenbottam TW, Stewart S, et al. (1996) Development of bronchiolitis obliterans syndrome in recipients of heart-lung transplantation – early risk factors. Transplantation 61: 560–566. - PubMed
-
- Trulock EP (1993) Management of lung transplant rejection. Chest 103: 1566–1576. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
