

The influence of a postdischarge intervention on reducing hospital readmissions in a Medicare population
- PMID: 23537154
- PMCID: PMC3771544
- DOI: 10.1089/pop.2012.0084
The influence of a postdischarge intervention on reducing hospital readmissions in a Medicare population
Abstract
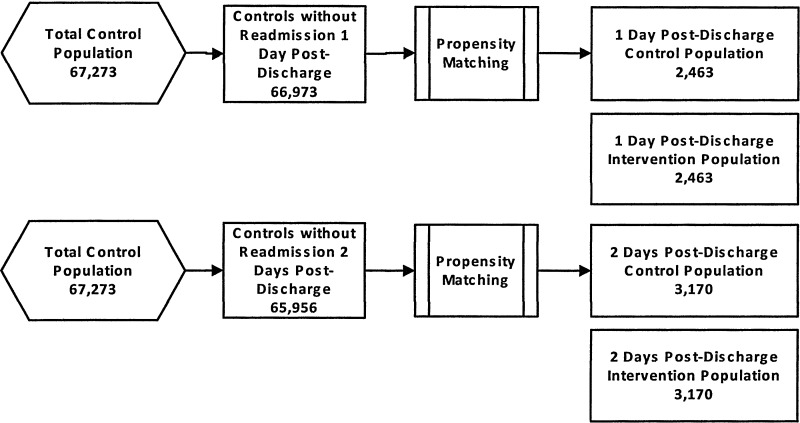
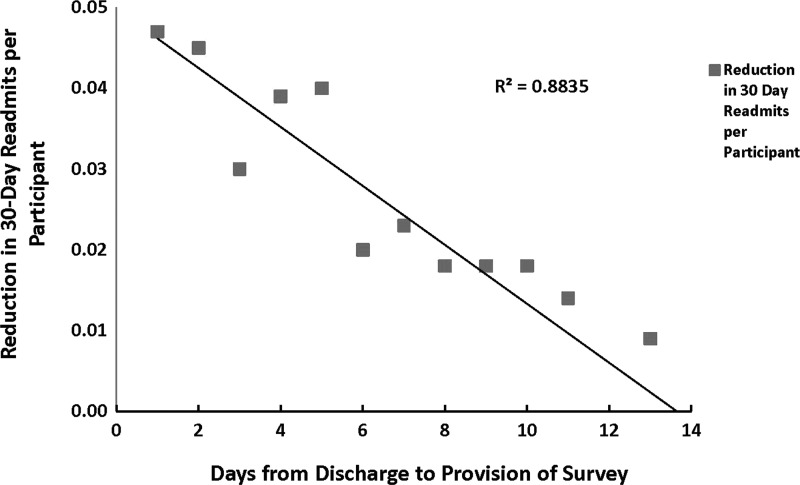
Hospital readmissions in the Medicare population may be related to a number of factors, including reoccurrence of illness, failure to understand or follow physician direction, or lack of follow-up care, among others. These readmissions significantly increase cost and utilization in this population, and are expected to increase with the projected growth in Medicare enrollment. The authors examined whether a postdischarge telephonic intervention for patients reduced 30-day hospital readmissions as compared to a matched control population. Postdischarge telephone calls were placed to patients after discharge from a hospital. Readmissions were monitored through health care claims data analysis. Of 48,538 Medicare members who received the intervention, 4504 (9.3%) were readmitted to the hospital within 30 days, as compared to 5598 controls (11.5%, P<0.0001). A direct correlation was observed between the timing of the intervention and the rate of readmission; the closer the intervention to the date of discharge the greater the reduction in number of readmissions. Furthermore, although emergency room visits were reduced in the intervention group as compared to controls (8.1% vs. 9.4%, P<0.0001), physician office visits increased (76.5% vs. 72.3%, P<0.0001), suggesting the intervention may have encouraged members to seek assistance leading to avoidance of readmission. As a group, overall cost savings were $499,458 for members who received the intervention, with $13,964,773 in savings to the health care plan. Support for patients after hospital discharge clearly affected hospital readmission and associated costs and warrants further development.
Figures
References
-
- Medicare Payment Advisory Commission. Washington, DC: Medicare Payment Advisory Commission; 2005. Report to the Congress: Reforming the Delivery System; pp. 83–103.
-
- Jencks SF. Williams MV. Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- Jencks SF. Defragmenting care. Ann Intern Med. 2010;153:757–758. - PubMed
-
- Grimmer KA. Moss JR. Gill TK. Discharge planning quality from the carer perspective. Qual Life Res. 2000;9:1005–1013. - PubMed
-
- Coleman EA. Boult C. Improving the quality of transitional care for persons with complex care needs. J Am Geriatr Soc. 2003;51:556–557. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
