

Electrical stimulation for chronic non-specific low back pain in a working-age population: a 12-week double blinded randomized controlled trial
- PMID: 23537462
- PMCID: PMC3626857
- DOI: 10.1186/1471-2474-14-117
Electrical stimulation for chronic non-specific low back pain in a working-age population: a 12-week double blinded randomized controlled trial
Abstract
Background: Non-invasive electrotherapy is commonly used for treatment of chronic low back pain. Evidence for efficacy of most electrotherapy modalities is weak or lacking. This study aims to execute a high-quality, double-blinded randomized controlled clinical trial comparing 1) H-Wave(®) Device stimulation plus usual care with 2) transcutaneous electrical nerve stimulation (TENS) plus usual care, and 3) Sham electrotherapy plus usual care to determine comparative efficacy for treatment of chronic non-specific low back pain patients.
Patients: Chronic non-specific low back pain patients between ages of 18-65 years, with pain of at least 3 months duration and minimal current 5/10 VAS pain. Patients will have no significant signs or symptoms of lumbosacral nerve impingement, malignancy, spinal stenosis, or mood disorders.
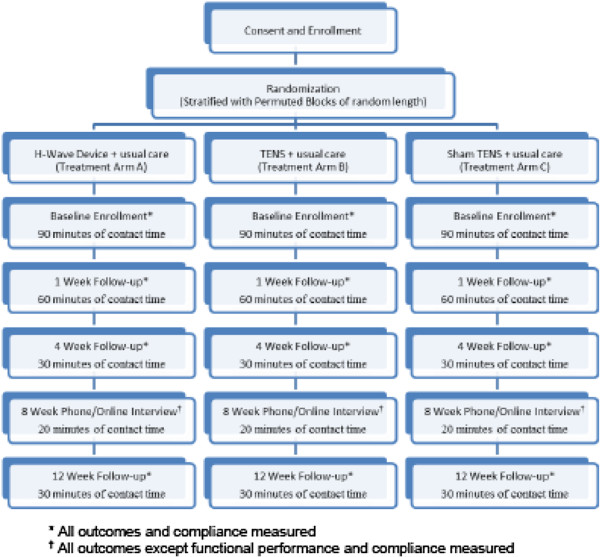
Study design: Double blind RCT with 3 arms and 38 subjects per arm. Randomization by permuted blocks of random length, stratified by Workers Compensation claim (yes vs. no), and use of opioids. The null hypothesis of this study is that there are no statistically significant differences in functional improvement between treatment types during and at the end of a 12-week week treatment period.
Data collection: Subjective data will be collected using Filemaker Pro™ database management collection tools. Objective data will be obtained through functional assessments. Data will be collected at enrollment and at 1, 4, 8, and 12 weeks for each participant by a blinded assessor.
Interventions: H-Wave(®) device stimulation (Intervention A) plus usual care, transcutaneous electrical nerve stimulation (TENS) (Intervention B) plus usual care, and sham electrotherapy plus usual care (control). Each treatment arm will have identical numbers of visits (4) and researcher contact time (approximately 15 hours).
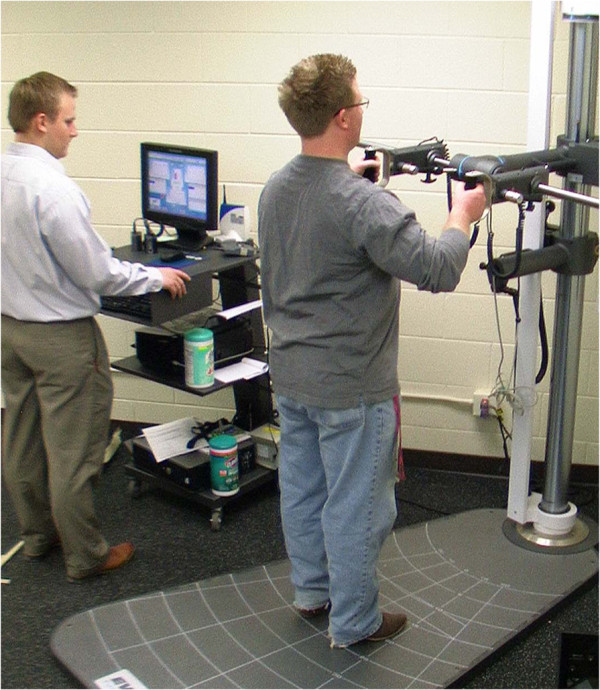
Primary outcome measure: Oswestry Disability Index. Secondary measures include: Rowland Morris Instrument, VAS pain score, functional evaluation including strength when pushing and pulling, pain free range of motion in flexion and extension. Outcome measures assessed at baseline, 1, 4, 8, and 12 weeks. Treatment failure will be defined if patient terminates assigned treatment arm for non-efficacy or undergoes invasive procedure or other excluded cointerventions. Data will be analyzed using intention-to-treat analysis and adjusted for covariates related to LBP (e.g. age) as needed.
Discussion: Study strengths include complex randomization, treatment group allocation concealment, double blinding, controlling for co-interventions, rigorous inclusion criteria, assessment of compliance, plans for limiting dropout, identical assessment methods and timing for each treatment arm, and planned intention-to-treat analyses.
Figures
Similar articles
-
Analgesic efficacy of cerebral and peripheral electrical stimulation in chronic nonspecific low back pain: a randomized, double-blind, factorial clinical trial.BMC Musculoskelet Disord. 2015 Jan 31;16(1):7. doi: 10.1186/s12891-015-0461-1. BMC Musculoskelet Disord. 2015. PMID: 25636503 Free PMC article. Clinical Trial.
-
Efficacy of Electronic Acupuncture Shoes for Chronic Low Back Pain: Double-Blinded Randomized Controlled Trial.J Med Internet Res. 2020 Oct 26;22(10):e22324. doi: 10.2196/22324. J Med Internet Res. 2020. PMID: 33104004 Free PMC article. Clinical Trial.
-
A Retrospective Analysis of 25 Cases With Peripheral Nerve Field Stimulation for Chronic Low Back Pain and the Predictive Value of Transcutaneous Electrical Nerve Stimulation for Patient Selection.Neuromodulation. 2019 Jul;22(5):607-614. doi: 10.1111/ner.12890. Epub 2018 Dec 7. Neuromodulation. 2019. PMID: 30548104
-
Literature Review and Meta-Analysis of Transcutaneous Electrical Nerve Stimulation in Treating Chronic Back Pain.Reg Anesth Pain Med. 2018 May;43(4):425-433. doi: 10.1097/AAP.0000000000000740. Reg Anesth Pain Med. 2018. PMID: 29394211 Free PMC article.
-
A Meta-Analysis of Transcutaneous Electrical Nerve Stimulation for Chronic Low Back Pain.Surg Technol Int. 2016 Apr;28:296-302. Surg Technol Int. 2016. PMID: 27042787 Review.
Cited by
-
Clinical and Quality of Life Benefits for End-Stage Workers' Compensation Chronic Pain Claimants following H-Wave® Device Stimulation: A Retrospective Observational Study with Mean 2-Year Follow-Up.J Clin Med. 2023 Feb 1;12(3):1148. doi: 10.3390/jcm12031148. J Clin Med. 2023. PMID: 36769795 Free PMC article.
-
Monochromatic Infrared Photo Energy Versus Low Level Laser Therapy in Chronic Low Back Pain.J Lasers Med Sci. 2015 Fall;6(4):157-61. doi: 10.15171/jlms.2015.11. Epub 2015 Oct 27. J Lasers Med Sci. 2015. PMID: 26705460 Free PMC article.
-
Effect of pulsed electromagnetic field on nonspecific low back pain patients: a randomized controlled trial.Braz J Phys Ther. 2019 May-Jun;23(3):244-249. doi: 10.1016/j.bjpt.2018.08.004. Epub 2018 Aug 21. Braz J Phys Ther. 2019. PMID: 30177406 Free PMC article. Clinical Trial.
-
Characterising the Features of 381 Clinical Studies Evaluating Transcutaneous Electrical Nerve Stimulation (TENS) for Pain Relief: A Secondary Analysis of the Meta-TENS Study to Improve Future Research.Medicina (Kaunas). 2022 Jun 14;58(6):803. doi: 10.3390/medicina58060803. Medicina (Kaunas). 2022. PMID: 35744066 Free PMC article. Review.
-
Effects of transcutaneous electrical nerve stimulation on pain in patients with spinal cord injury: a randomized controlled trial.J Phys Ther Sci. 2015 Jan;27(1):23-5. doi: 10.1589/jpts.27.23. Epub 2015 Jan 9. J Phys Ther Sci. 2015. PMID: 25642029 Free PMC article.
References
-
- Deyo RA. Promises and limitations of the Patient Outcome Research Teams: the low-back pain example. Proc Assoc Am Physicians. 1995;107(3):324–328. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
