

Pediatric sepsis: challenges and adjunctive therapies
- PMID: 23537672
- PMCID: PMC3612267
- DOI: 10.1016/j.ccc.2012.11.003
Pediatric sepsis: challenges and adjunctive therapies
Abstract
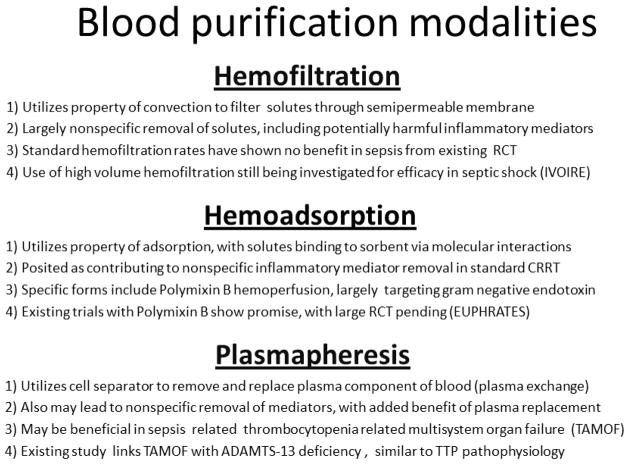
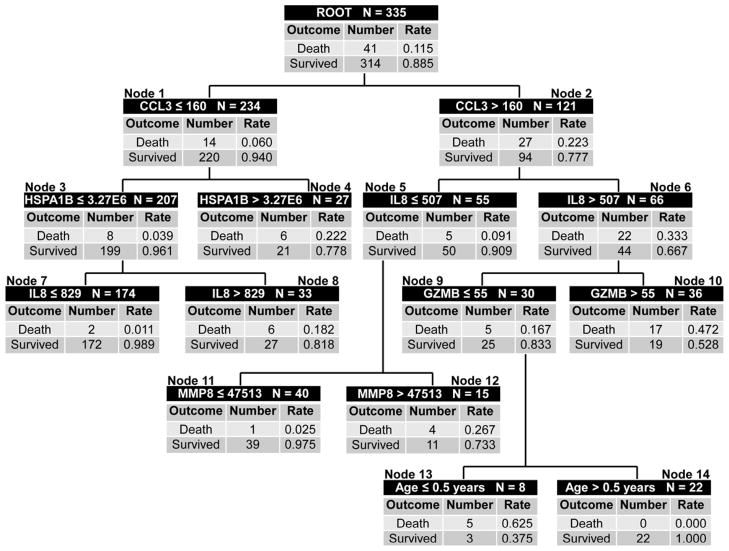
Sepsis remains an important challenge in pediatric critical care medicine. This review provides an appraisal of adjunctive therapies for sepsis and highlights opportunities for meeting selected challenges in the field. Future clinical studies should address long-term and functional outcomes as well as acute outcomes. Potential adjunctive therapies such as corticosteroids, hemofiltration, hemoadsorption, and plasmapheresis may have important roles, but still require formal and more rigorous testing by way of clinical trials. Finally, the design of future clinical trials should consider novel approaches for stratifying outcome risks as a means of improving the risk-to-benefit ratio of experimental therapies.
Published by Elsevier Inc.
Figures
References
-
- Wong HR, Nowak JE, Standage S, de Oliveira CF. Sepsis and Septic Shock. In: Fuhrman BP, Zimmerman JJ, editors. Pediatric Critical Care Medicine. 4. St. Louis: Mosby; 2011. pp. 1413–1429.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
