

Community viral load as a measure for assessment of HIV treatment as prevention
- PMID: 23537801
- PMCID: PMC4512165
- DOI: 10.1016/S1473-3099(12)70314-6
Community viral load as a measure for assessment of HIV treatment as prevention
Abstract
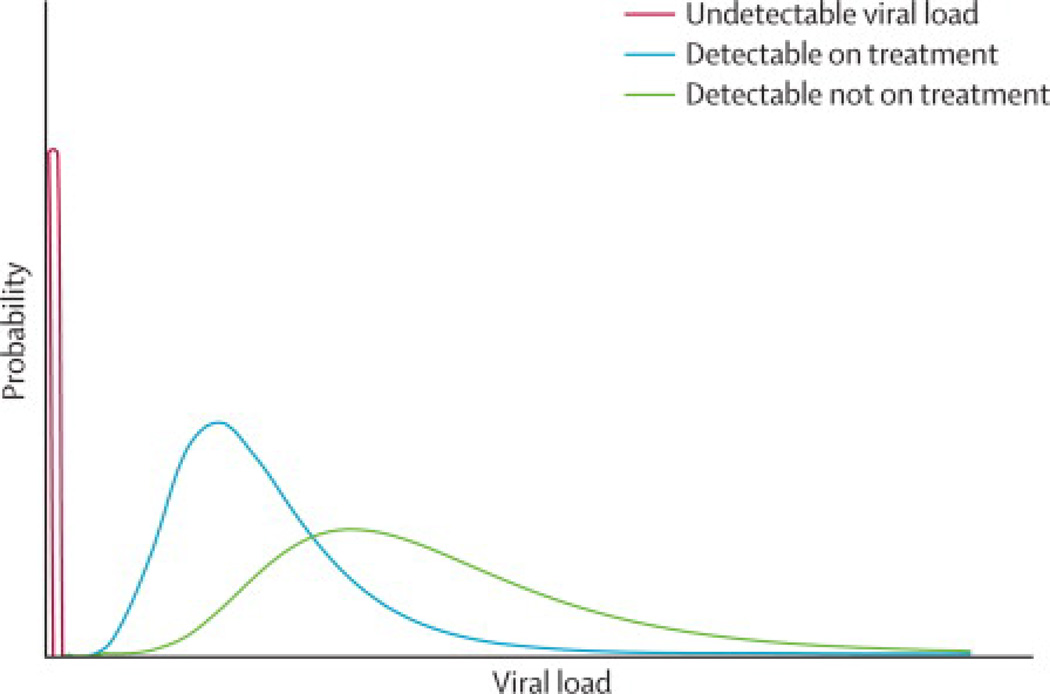
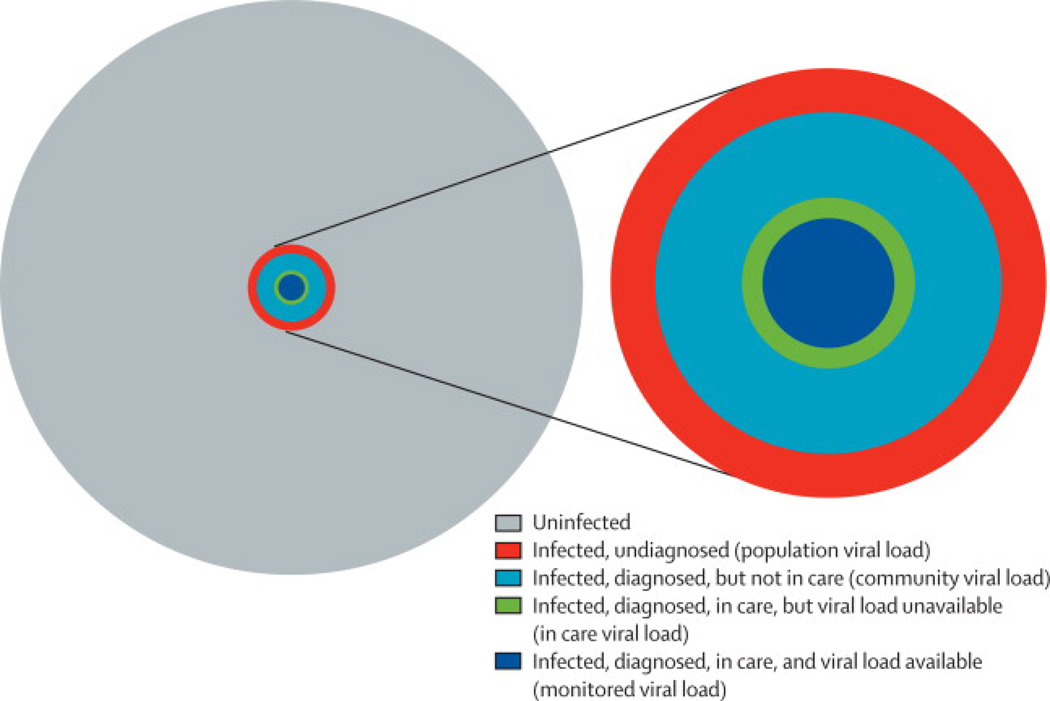
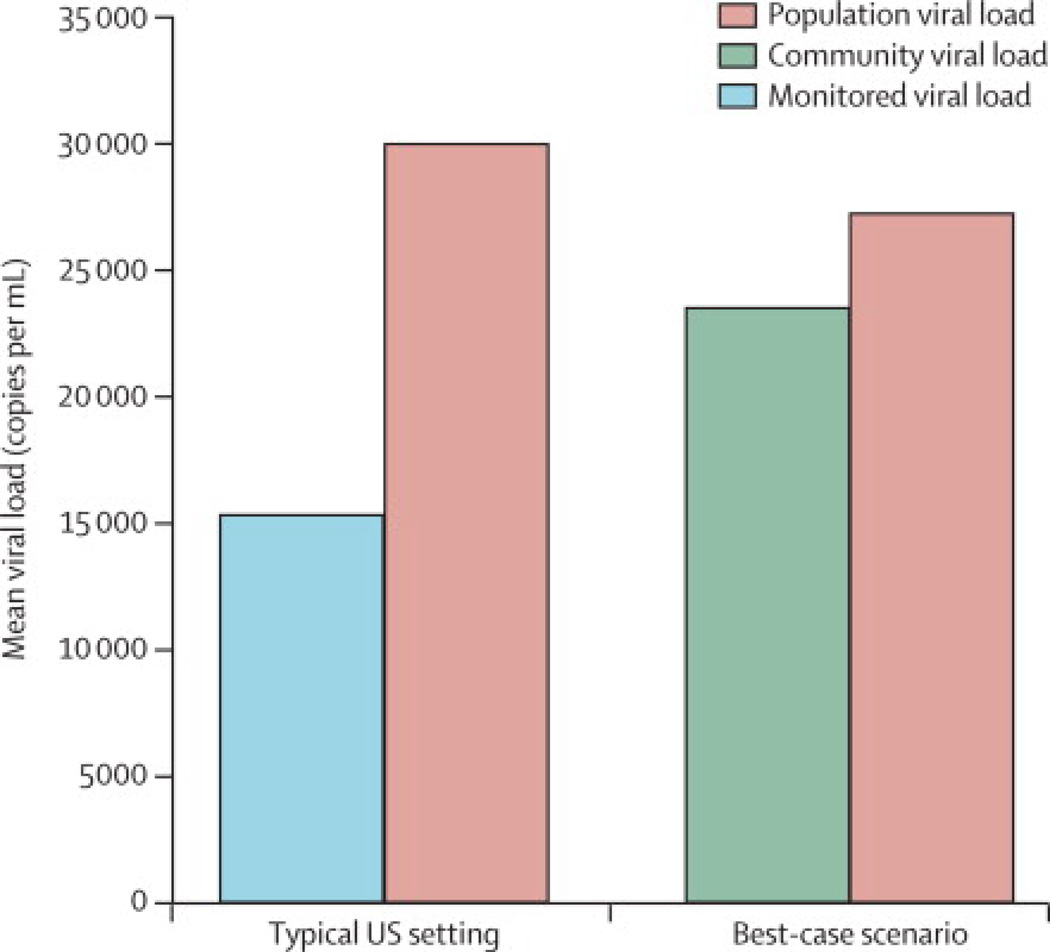
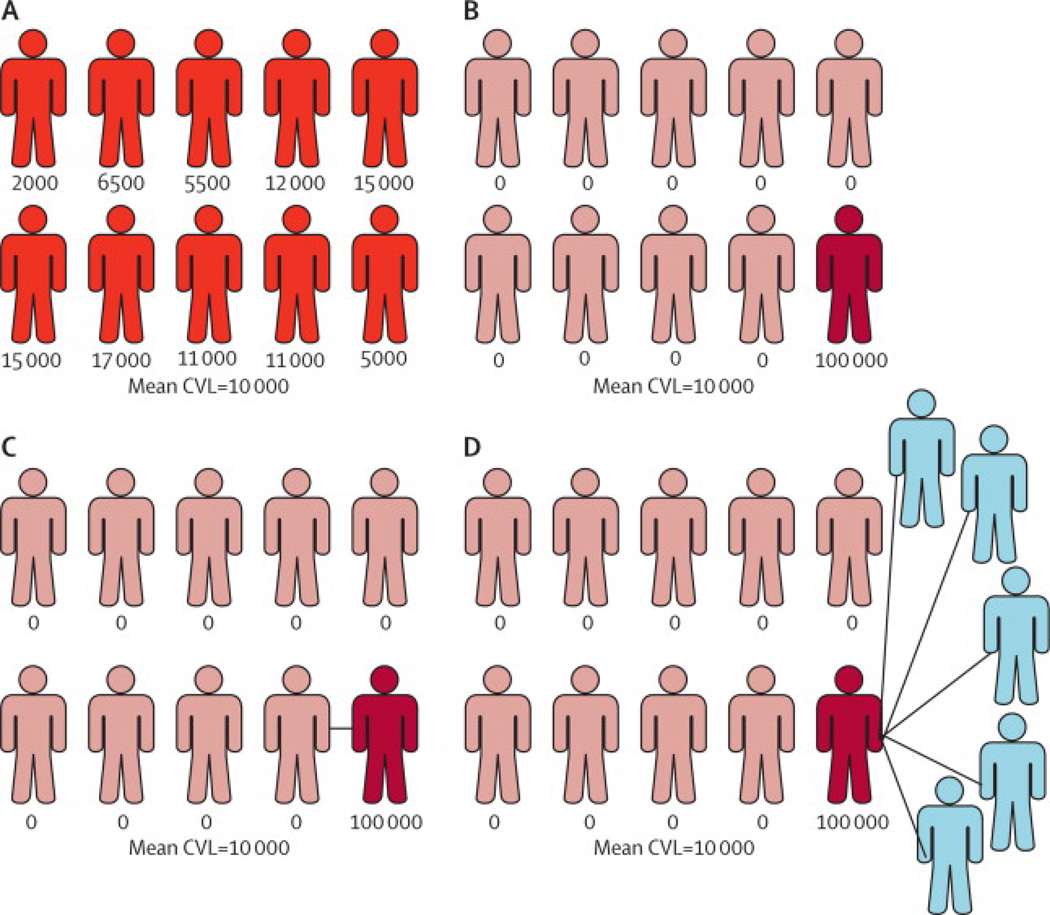
Community viral load, defined as an aggregation of individual viral loads of people infected with HIV in a specific community, has been proposed as a useful measure to monitor HIV treatment uptake and quantify its effect on transmission. The first reports of community viral load were published in 2009, and the measure was subsequently incorporated into the US National HIV/AIDS Strategy. Although intuitively an appealing strategy, measurement of community viral load has several theoretical limitations and biases that need further assessment, which can be grouped into four categories: issues of selection and measurement, the importance of HIV prevalence in determining the potential for ongoing HIV transmission, interpretation of community viral load and its effect on ongoing HIV transmission in a community, and the ecological fallacy (ie, ecological bias). These issues need careful assessment as community viral load is being considered as a public health measurement to assess the effect of HIV care on prevention.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
References
-
- Castel AD, Befus M, Willis S, et al. Use of the community viral load as a population-based biomarker of HIV burden. AIDS. 2012;26:345–353. - PubMed
-
- Jain V, Liegler T, Chamie G, et al. CROI. Seattle, WA: 2012. Mar 5–8, Assessment of community viral load using a fingerprick-based blood collection method: Uganda. 2012, 2012;
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
