

Simple risk model predicts incidence of atrial fibrillation in a racially and geographically diverse population: the CHARGE-AF consortium
- PMID: 23537808
- PMCID: PMC3647274
- DOI: 10.1161/JAHA.112.000102
Simple risk model predicts incidence of atrial fibrillation in a racially and geographically diverse population: the CHARGE-AF consortium
Abstract
Background: Tools for the prediction of atrial fibrillation (AF) may identify high-risk individuals more likely to benefit from preventive interventions and serve as a benchmark to test novel putative risk factors.
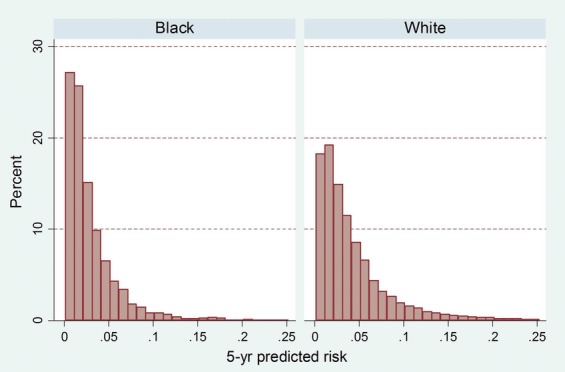
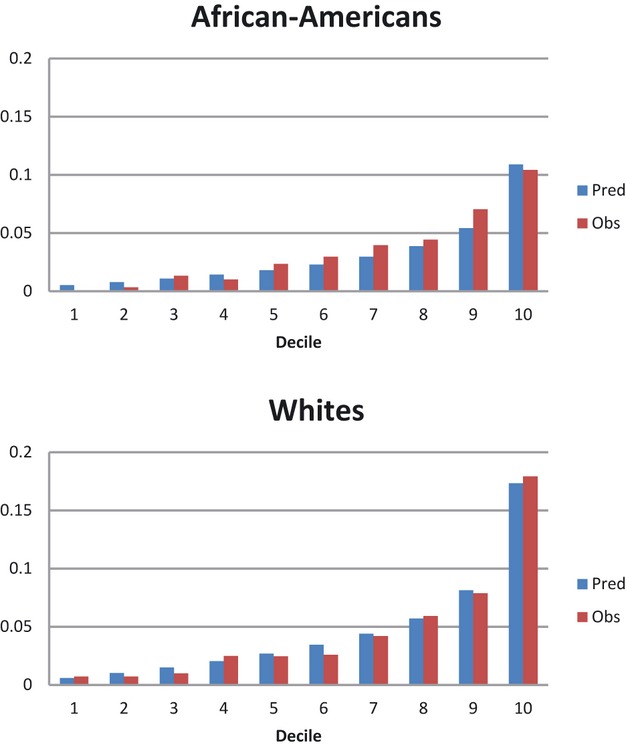
Methods and results: Individual-level data from 3 large cohorts in the United States (Atherosclerosis Risk in Communities [ARIC] study, the Cardiovascular Health Study [CHS], and the Framingham Heart Study [FHS]), including 18 556 men and women aged 46 to 94 years (19% African Americans, 81% whites) were pooled to derive predictive models for AF using clinical variables. Validation of the derived models was performed in 7672 participants from the Age, Gene and Environment-Reykjavik study (AGES) and the Rotterdam Study (RS). The analysis included 1186 incident AF cases in the derivation cohorts and 585 in the validation cohorts. A simple 5-year predictive model including the variables age, race, height, weight, systolic and diastolic blood pressure, current smoking, use of antihypertensive medication, diabetes, and history of myocardial infarction and heart failure had good discrimination (C-statistic, 0.765; 95% CI, 0.748 to 0.781). Addition of variables from the electrocardiogram did not improve the overall model discrimination (C-statistic, 0.767; 95% CI, 0.750 to 0.783; categorical net reclassification improvement, -0.0032; 95% CI, -0.0178 to 0.0113). In the validation cohorts, discrimination was acceptable (AGES C-statistic, 0.664; 95% CI, 0.632 to 0.697 and RS C-statistic, 0.705; 95% CI, 0.664 to 0.747) and calibration was adequate.
Conclusion: A risk model including variables readily available in primary care settings adequately predicted AF in diverse populations from the United States and Europe.
Figures
References
-
- Go AS, Hylek EM, Phillips KA, Chang YC, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults. National implications for rhythm management and stroke prevention: the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001; 285:2370-2375 - PubMed
-
- Wolf PA, Mitchell JB, Baker CS, Kannel WB, D'Agostino RB. Impact of atrial fibrillation on mortality, stroke, and medical costs. Arch Intern Med. 1998; 158:229-234 - PubMed
-
- Kim MH, Johnston SS, Chu B‐C, Dalal MR, Schulman KL. Estimation of total incremental health care costs in patients with atrial fibrillation in the United States. Circ Cardiovasc Qual Outcomes. 2011; 4:313-320 - PubMed
-
- Schnabel RB, Sullivan LM, Levy D, Pencina MJ, Massaro JM, D'Agostino RB, Sr, Newton‐Cheh C, Yamamoto JF, Magnani JW, Tadros TM, Kannel WB, Wang TJ, Ellinor PT, Wolf PA, Vasan RS, Benjamin EJ. Development of a risk score for atrial fibrillation (Framingham Heart Study): a community‐based cohort study. Lancet. 2009; 373:739-745 - PMC - PubMed
-
- Schnabel RB, Aspelund T, Li G, Sullivan LM, Suchy‐Dicey A, Harris TB, Pencina MJ, D'Agostino RB, Sr, Levy D, Kannel WB, Wang TJ, Kronmal RA, Wolf PA, Burke GL, Launer LJ, Vasan RS, Psaty BM, Benjamin EJ, Gudnason V, Heckbert SR. Validation of an atrial fibrillation risk algorithm in whites and African‐Americans. Arch Intern Med. 2010; 170:1909-1917 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- 1RC1HL101056/HL/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- RC1 HL099452/HL/NHLBI NIH HHS/United States
- R01 HL088456/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- 1R21HL106092/HL/NHLBI NIH HHS/United States
- R21 HL106092/HL/NHLBI NIH HHS/United States
- K24 HL105780/HL/NHLBI NIH HHS/United States
- RC1HL099452/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- R01HL088456/HL/NHLBI NIH HHS/United States
- AG-15928/AG/NIA NIH HHS/United States
- UL1 TR000161/TR/NCATS NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- N01-HC 25195/HC/NHLBI NIH HHS/United States
- AG-20098/AG/NIA NIH HHS/United States
- RC1 HL101056/HL/NHLBI NIH HHS/United States
- R01 HL105756/HL/NHLBI NIH HHS/United States
- RC1HL101056/HL/NHLBI NIH HHS/United States
- AG-027058/AG/NIA NIH HHS/United States
- R01 HL102214/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- KL2 TR000160/TR/NCATS NIH HHS/United States
- 6R01-NS 17950/NS/NINDS NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- N01-AG-12100/AG/NIA NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HL080295/HL/NHLBI NIH HHS/United States
- 1R01HL102214/HL/NHLBI NIH HHS/United States
- 1R01AG028321/AG/NIA NIH HHS/United States
- AG-023629/AG/NIA NIH HHS/United States
- 1R01HL092577/HL/NHLBI NIH HHS/United States
- R01 AG028321/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
