

Long-term outcomes of catheter ablation of atrial fibrillation: a systematic review and meta-analysis
- PMID: 23537812
- PMCID: PMC3647286
- DOI: 10.1161/JAHA.112.004549
Long-term outcomes of catheter ablation of atrial fibrillation: a systematic review and meta-analysis
Abstract
Background: In the past decade, catheter ablation has become an established therapy for symptomatic atrial fibrillation (AF). Until very recently, few data have been available to guide the clinical community on the outcomes of AF ablation at ≥3 years of follow-up. We aimed to systematically review the medical literature to evaluate the long-term outcomes of AF ablation.
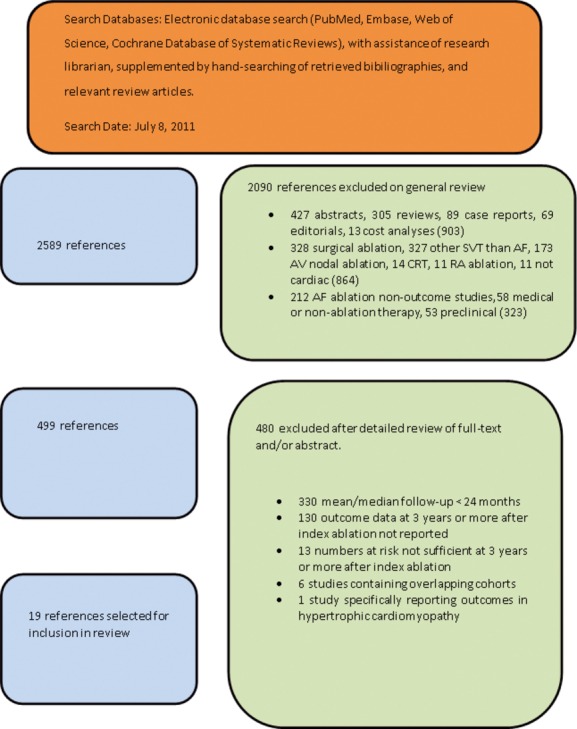
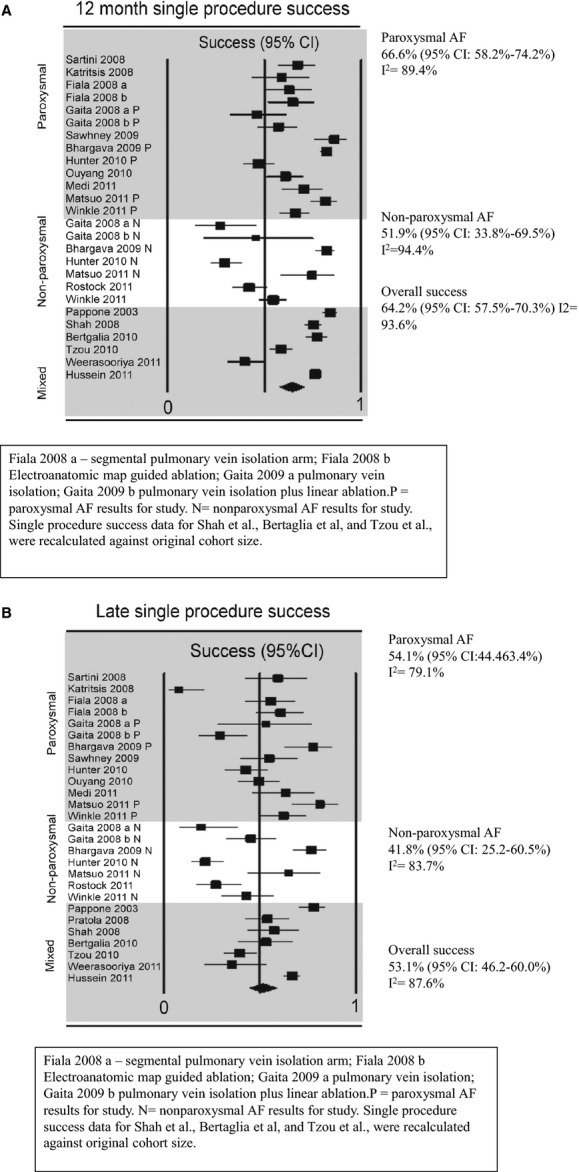
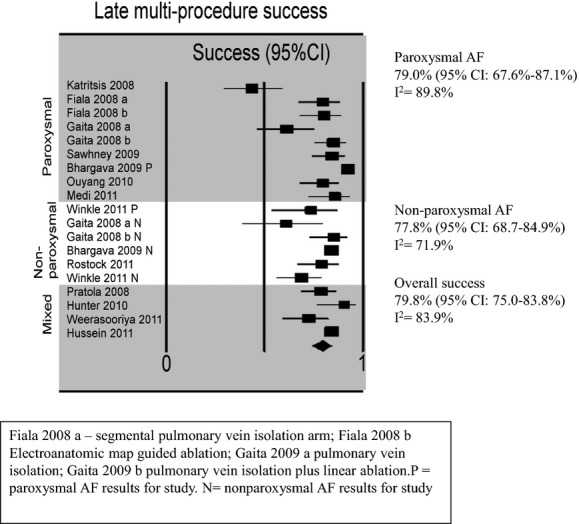
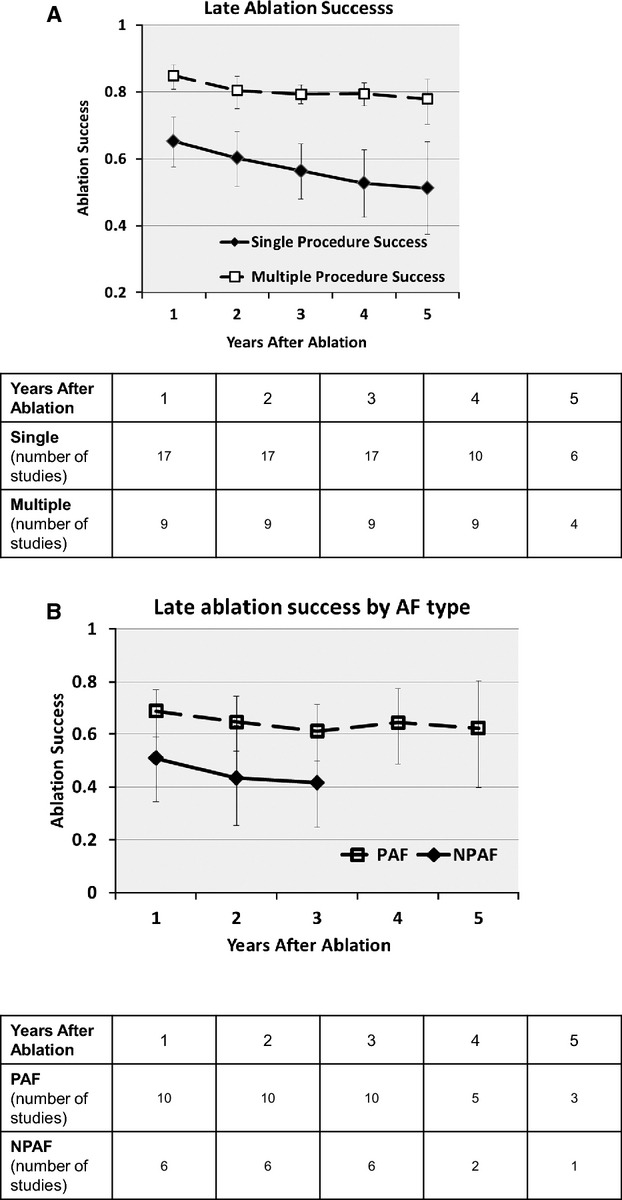
Methods and results: A structured electronic database search (PubMed, Embase, Web of Science, Cochrane) of the scientific literature was performed for studies describing outcomes at ≥3 years after AF ablation, with a mean follow-up of ≥24 months after the index procedure. The following data were extracted: (1) single-procedure success, (2) multiple-procedure success, and (3) requirement for repeat procedures. Data were extracted from 19 studies, including 6167 patients undergoing AF ablation. Single-procedure freedom from atrial arrhythmia at long-term follow-up was 53.1% (95% CI 46.2% to 60.0%) overall, 54.1% (95% CI 44.4% to 63.4%) in paroxysmal AF, and 41.8% (95% CI 25.2% to 60.5%) in nonparoxysmal AF. Substantial heterogeneity (I(2)>50%) was noted for single-procedure outcomes. With multiple procedures, the long-term success rate was 79.8% (95% CI 75.0% to 83.8%) overall, with significant heterogeneity (I(2)>50%).The average number of procedures per patient was 1.51 (95% CI 1.36 to 1.67).
Conclusions: Catheter ablation is an effective and durable long-term therapeutic strategy for some AF patients. Although significant heterogeneity is seen with single procedures, long-term freedom from atrial arrhythmia can be achieved in some patients, but multiple procedures may be required.
Figures
References
-
- Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998; 339:659-666 - PubMed
-
- Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, Crijns HJ, Damiano RJ, Jr, Davies DW, DiMarco J, Edgerton J, Ellenbogen K, Ezekowitz MD, Haines DE, Haissaguerre M, Hindricks G, Iesaka Y, Jackman W, Jalife J, Jais P, Kalman J, Keane D, Kim YH, Kirchhof P, Klein G, Kottkamp H, Kumagai K, Lindsay BD, Mansour M, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Nakagawa H, Natale A, Nattel S, Packer DL, Pappone C, Prystowsky E, Raviele A, Reddy V, Ruskin JN, Shemin RJ, Tsao HM, Wilber D. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2012; 9:632-696.e621
-
- Bunch TJ, Day JD. Achieving favorable very long‐term outcomes after catheter ablation for atrial fibrillation: an exciting adventure or delusional quest? J Cardiovasc Electrophysiol. 2011; 22:1215-1216 - PubMed
-
- Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, Van Gelder IC, Al‐Attar N, Hindricks G, Prendergast B, Heidbuchel H, Alfieri O, Angelini A, Atar D, Colonna P, De Caterina R, De Sutter J, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, Le Heuzey JY, Ponikowski P, Rutten FH. Guidelines for the management of atrial fibrillation. Eur Heart J. 2010; 31:2369-2429 - PubMed
-
- Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB. Meta‐analysis of observational studies in epidemiology: a proposal for reporting. Meta‐analysis of Observational Studies in Epidemiology (MOOSE) Group. JAMA. 2000; 283:2008-2012 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
