

Acquired cystic fibrosis transmembrane conductance regulator dysfunction in the lower airways in COPD
- PMID: 23538783
- PMCID: PMC3734887
- DOI: 10.1378/chest.13-0274
Acquired cystic fibrosis transmembrane conductance regulator dysfunction in the lower airways in COPD
Abstract
Background: Cigarette smoke and smoking-induced inflammation decrease cystic fibrosis transmembrane conductance regulator (CFTR) activity and mucociliary transport in the nasal airway and cultured bronchial epithelial cells. This raises the possibility that lower airway CFTR dysfunction may contribute to the pathophysiology of COPD. We compared lower airway CFTR activity in current and former smokers with COPD, current smokers without COPD, and lifelong nonsmokers to examine the relationships between clinical characteristics and CFTR expression and function.
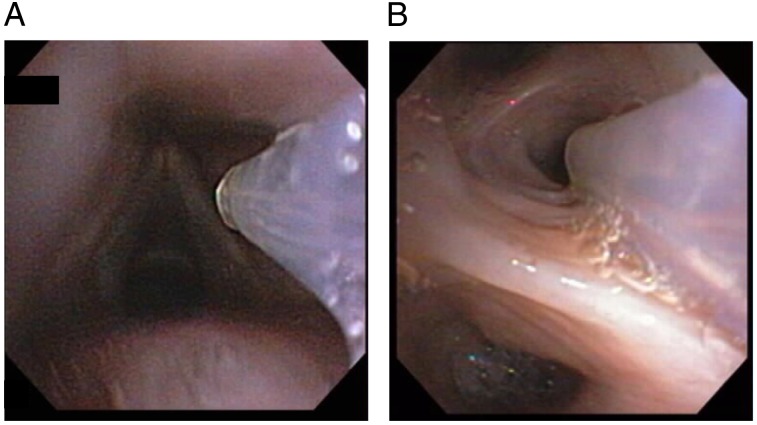
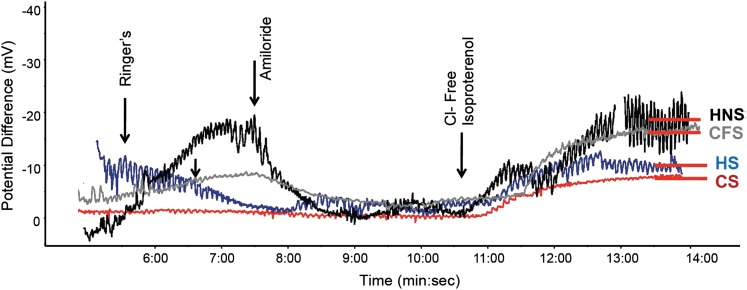
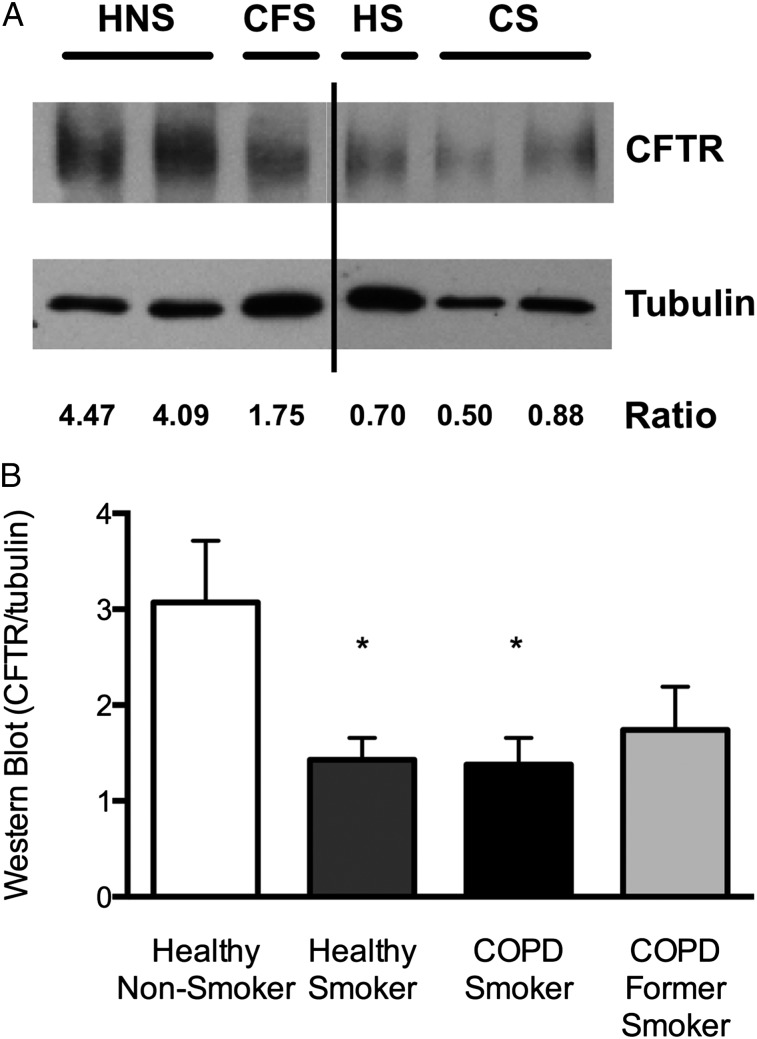
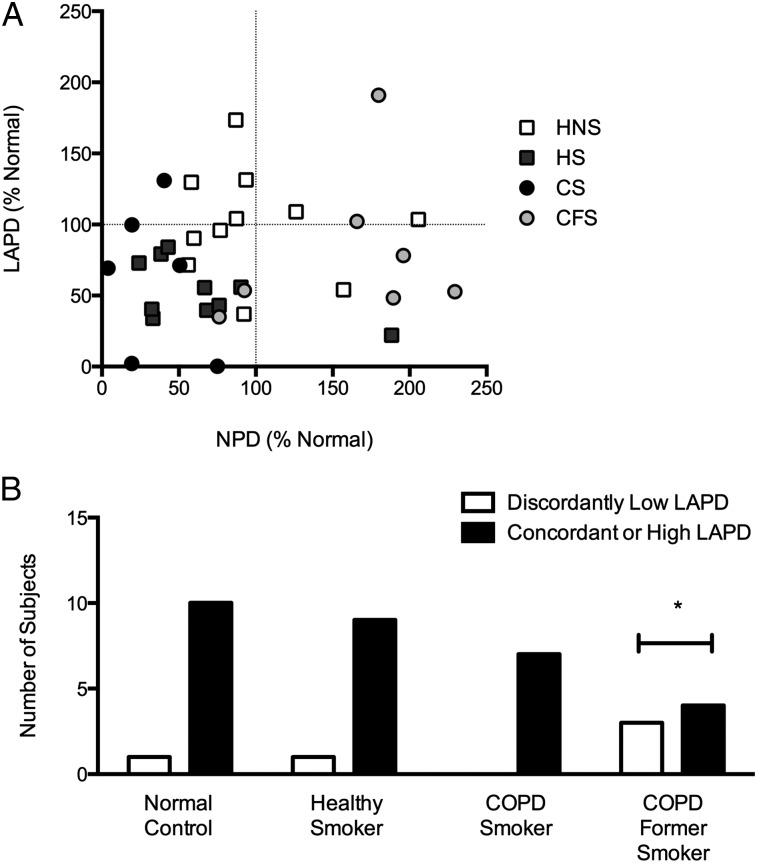
Methods: Demographic, spirometry, and symptom questionnaire data were collected. CFTR activity was determined by nasal potential difference (NPD) and lower airway potential difference (LAPD) assays. The primary measure of CFTR function was the total change in chloride transport (Δchloride-free isoproterenol). CFTR protein expression in endobronchial biopsy specimens was measured by Western blot.
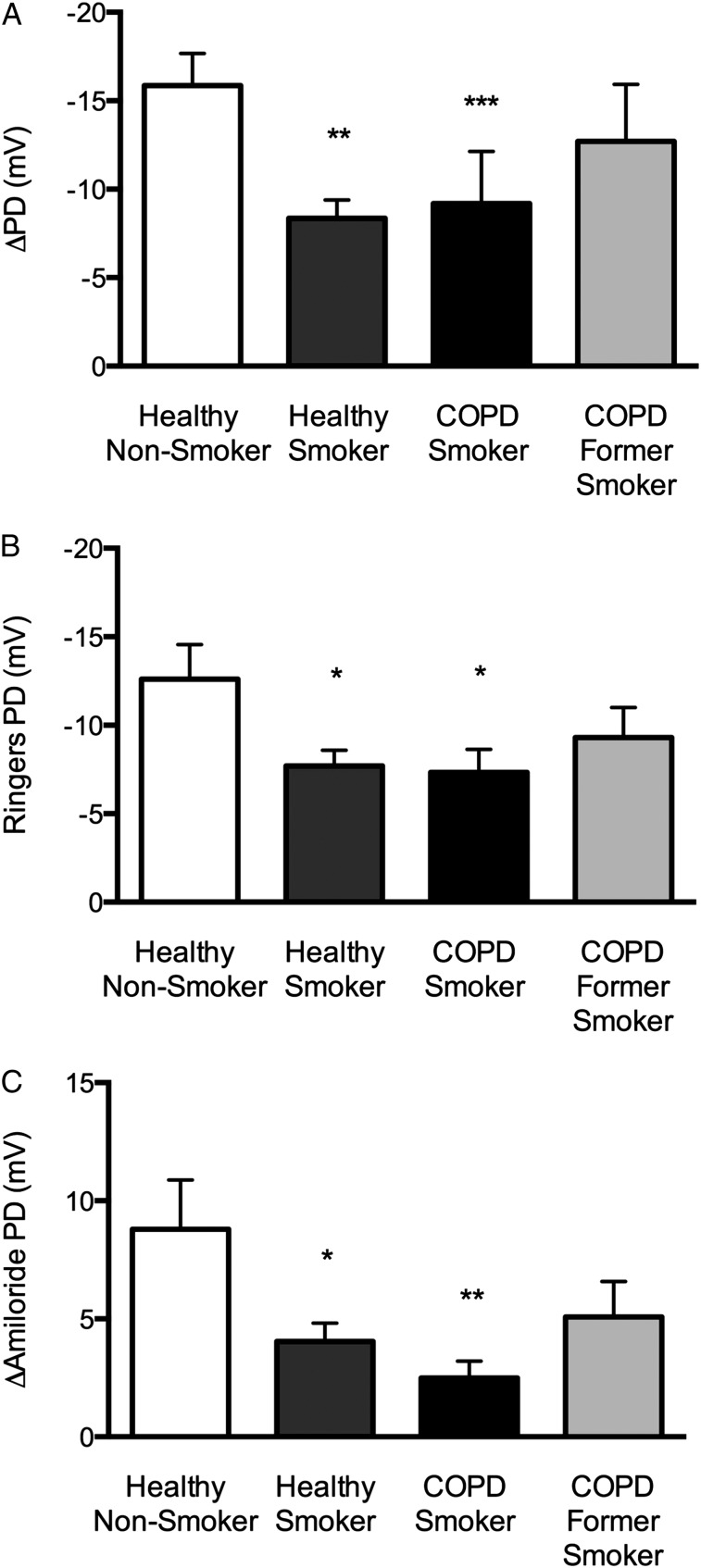
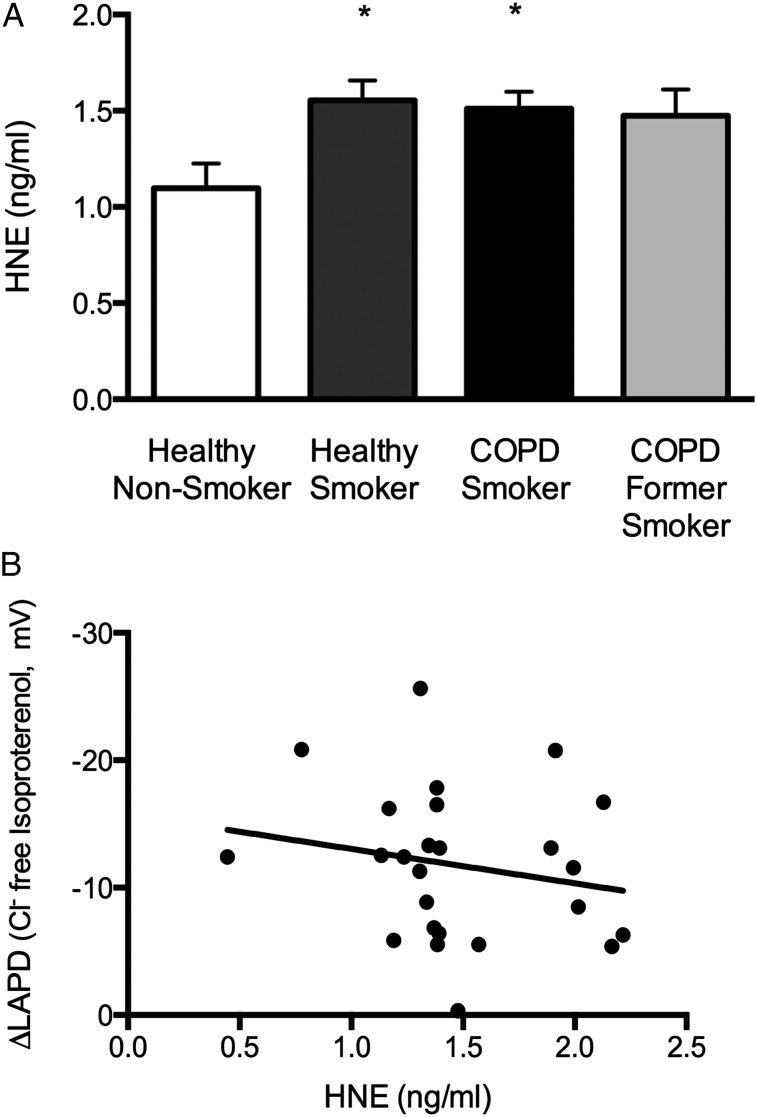
Results: Compared with healthy nonsmokers (n = 11), current smokers (n = 17) showed a significant reduction in LAPD CFTR activity (Δchloride-free isoproterenol, -8.70 mV vs -15.9 mV; P = .003). Similar reductions were observed in smokers with and without COPD. Former smokers with COPD (n = 7) showed a nonsignificant reduction in chloride conductance (-12.7 mV). A similar pattern was observed for CFTR protein expression. Univariate analysis demonstrated correlations between LAPD CFTR activity and current smoking, the presence of chronic bronchitis, and dyspnea scores.
Conclusions: Smokers with and without COPD have reduced lower airway CFTR activity compared with healthy nonsmokers, and this finding correlates with disease phenotype. Acquired CFTR dysfunction may contribute to COPD pathogenesis.
Figures
References
-
- National Heart, Lung, and Blood Institute, National Institutes of Health Morbidity and Mortality: 2007 Chart Book on Cardiovascular, Lung and Blood Diseases. Bethesda, MD: National Institutes of Health; 2007:17
-
- Centers for Disease Control and Prevention National Center for Health Statistics. Deaths: final data for 2007. Final Vital Stat Rep. 2010;58(19). - PubMed
-
- Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645-2653 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
