

Effect of routine controlled cord traction as part of the active management of the third stage of labour on postpartum haemorrhage: multicentre randomised controlled trial (TRACOR)
- PMID: 23538918
- PMCID: PMC3610557
- DOI: 10.1136/bmj.f1541
Effect of routine controlled cord traction as part of the active management of the third stage of labour on postpartum haemorrhage: multicentre randomised controlled trial (TRACOR)
Erratum in
- BMJ. 2013;346:f2542
- BMJ.2013;347:f6619
Abstract
Objective: To assess the impact of controlled cord traction on the incidence of postpartum haemorrhage and other characteristics of the third stage of labour in a high resource setting.
Design: Randomised controlled trial.
Setting: Five university hospital maternity units in France.
Participants: Women aged 18 or more with a singleton fetus at 35 or more weeks' gestation and planned vaginal delivery.
Interventions: Women were randomly assigned to management of the third stage of labour by controlled cord traction or standard placenta expulsion (awaiting spontaneous placental separation before facilitating expulsion). Women in both arms received prophylactic oxytocin just after birth.
Main outcome measure: Incidence of postpartum haemorrhage ≥ 500 mL as measured in a collector bag.
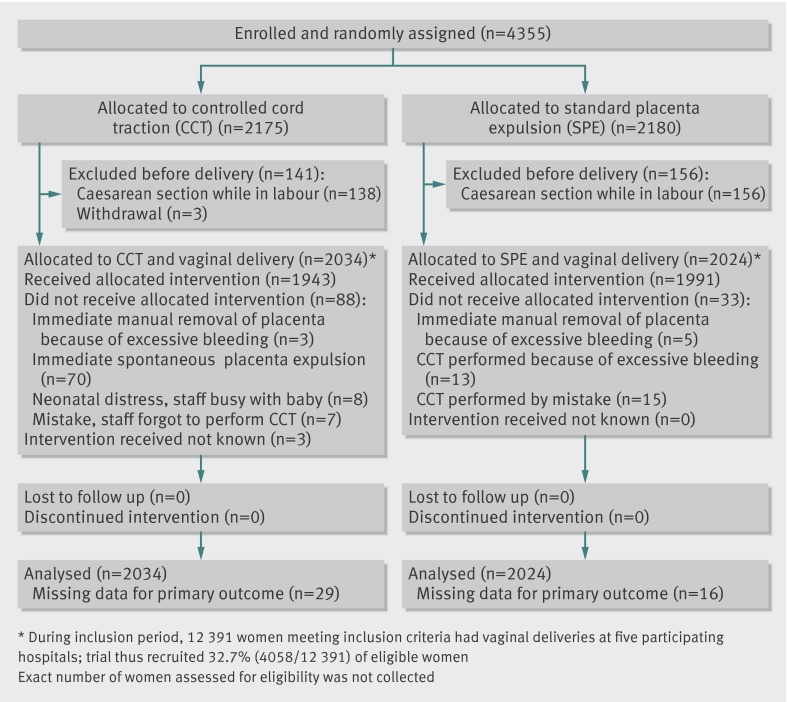
Results: The incidence of postpartum haemorrhage did not differ between the controlled cord traction arm (9.8%, 196/2005) and standard placenta expulsion arm (10.3%, 206/2008): relative risk 0.95 (95% confidence interval 0.79 to 1.15). The need for manual removal of the placenta was significantly less frequent in the controlled cord traction arm (4.2%, 85/2033) compared with the standard placenta expulsion arm (6.1%, 123/2024): relative risk 0.69, 0.53 to 0.90); as was third stage of labour of more than 15 minutes (4.5%, 91/2030 and 14.3%, 289/2020, respectively): relative risk 0.31, 0.25 to 0.39. Women in the controlled cord traction arm reported a significantly lower intensity of pain and discomfort during the third stage than those in the standard placenta expulsion arm. No uterine inversion occurred in either arm.
Conclusions: In a high resource setting, the use of controlled cord traction for the management of placenta expulsion had no significant effect on the incidence of postpartum haemorrhage and other markers of postpartum blood loss. Evidence to recommend routine controlled cord traction for the management of placenta expulsion to prevent postpartum haemorrhage is therefore lacking.
Trial registration: ClinicalTrials.gov NCT01044082.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Comment in
-
What is new in postpartum hemorrhage? Best articles from the past year.Obstet Gynecol. 2013 Sep;122(3):693-4. doi: 10.1097/AOG.0b013e3182a2c357. Obstet Gynecol. 2013. PMID: 23921880
References
-
- Khan KS, Wojdyla D, Say L, Gulmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet 2006;367:1066-74. - PubMed
-
- Callaghan WM, Mackay AP, Berg CJ. Identification of severe maternal morbidity during delivery hospitalizations, United States, 1991-2003. Am J Obstet Gynecol 2008;199:133.e1-8. - PubMed
-
- Zhang WH, Alexander S, Bouvier-Colle MH, Macfarlane A. Incidence of severe pre-eclampsia, postpartum haemorrhage and sepsis as a surrogate marker for severe maternal morbidity in a European population-based study: the MOMS-B survey. BJOG 2005;112:89-96. - PubMed
-
- Zwart J, Richters J, Öry F, de Vries J, Bloermenkamp K, van Roosmalen J. Severe maternal morbidity during pregnancy, delivery and puerperium in the Netherlands: a nationwide population-based study of 371 000 pregnancies. BJOG 2008;115:842-50. - PubMed
-
- Brace V, Penney G, Hall M. Quantifying severe maternal morbidity: a Scottish population study. BJOG 2004;111:481-4. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases