

Idiopathic adult growth hormone deficiency
- PMID: 23539718
- PMCID: PMC3667267
- DOI: 10.1210/jc.2012-4012
Idiopathic adult growth hormone deficiency
Abstract
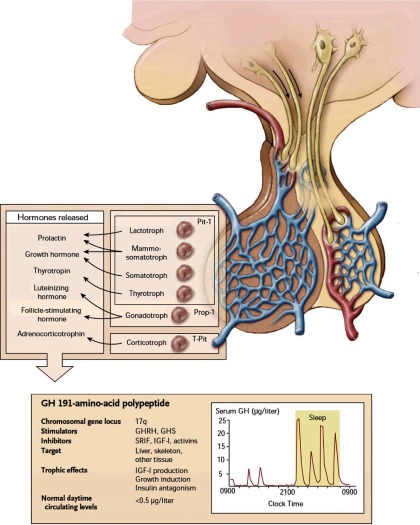
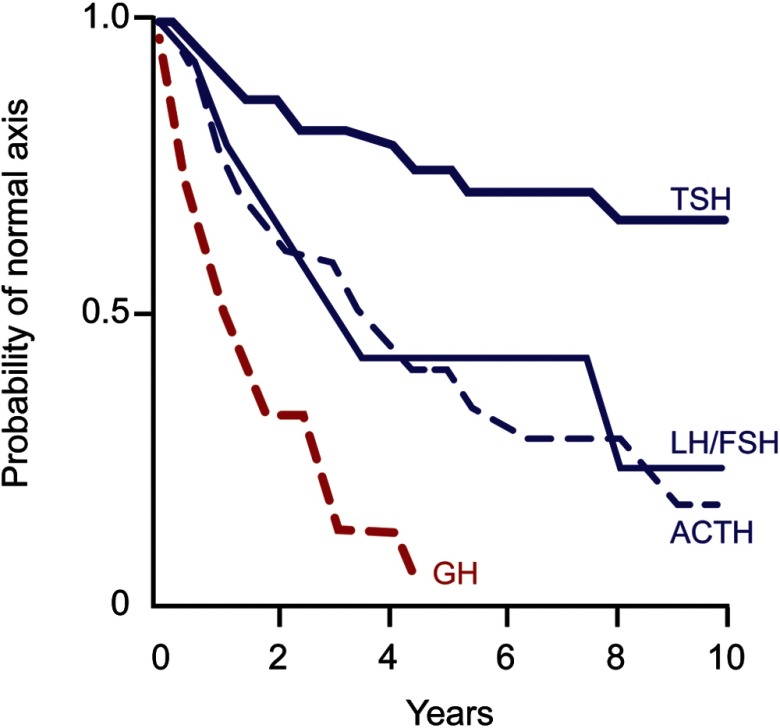
GH secretion is controlled by hypothalamic as well as intrapituitary and peripheral signals, all of which converge upon the somatotroph, resulting in integrated GH synthesis and secretion. Enabling an accurate diagnosis of idiopathic adult GH deficiency (IAGHD) is challenged by the pulsatility of GH secretion, provocative test result variability, and suboptimal GH assay standardization. The spectrum between attenuated GH secretion associated with the normal aging process and with obesity and truly well-defined IAGHD is not distinct and may mislead the diagnosis. Adult-onset GHD is mainly caused by an acquired pituitary deficiency, commonly including prior head/neck irradiation, or an expanding pituitary mass causing functional somatotroph compression. To what extent rare cryptic causes account for those patients seemingly classified as IAGHD is unclear. About 15% of patients with adult GHD and receiving GH replacement in open-label surveillance studies are reported as being due to an idiopathic cause. These patients may also reflect a pool of subjects with an as yet to be determined occult defect, or those with unclear or incomplete medical histories (including forgotten past sports head injury or motor vehicle accident). Therefore, submaximal diagnostic evaluation likely leads to an inadvertent diagnosis of IAGHD. In these latter cases, adherence to rigorous biochemical diagnostic criteria and etiology exclusion may result in reclassification of a subset of these patients to a distinct known acquired etiology, or as GH-replete. Accordingly, rigorously verified IAGHD likely comprises less than 10% of adult GHD patients, an already rare disorder. Regardless of etiology, patients with adult GHD, including those with IAGHD, exhibit a well-defined clinical phenotype including increased fat mass, loss of lean muscle mass, decreased bone mass, and enhanced cardiac morbidity. Definition of unique efficacy and dosing parameters for GH replacement and resultant therapeutic efficacy markers in true IAGHD requires prospective study.
Figures


Comment in
-
Idiopathic growth hormone deficiency in adults, Ben Johnson and the somatopause.J Clin Endocrinol Metab. 2013 Jun;98(6):2270-3. doi: 10.1210/jc.2013-2025. J Clin Endocrinol Metab. 2013. PMID: 23729014 No abstract available.
References
-
- Salomon F, Cuneo RC, Hesp R, Sonksen PH. The effects of treatment with recombinant human growth hormone on body composition and metabolism in adults with growth hormone deficiency. N Engl J Med. 1989;321:1797–1803 - PubMed
-
- Ho KK. Consensus guidelines for the diagnosis and treatment of adults with GH deficiency II: a statement of the GH Research Society in association with the European Society for Pediatric Endocrinology, Lawson Wilkins Society, European Society of Endocrinology, Japan Endocrine Society, and Endocrine Society of Australia. Eur J Endocrinol. 2007;157:695–700 - PubMed
-
- Hoffman AR, Kuntze JE, Baptista J, et al. Growth hormone (GH) replacement therapy in adult-onset GH deficiency: effects on body composition in men and women in a double-blind, randomized, placebo-controlled trial. J Clin Endocrinol Metab. 2004;89:2048–2056 - PubMed
-
- Molitch ME, Clemmons DR, Malozowski S, Merriam GR, Vance ML; Endocrine Society Evaluation and treatment of adult growth hormone deficiency: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2011;96:1587–1609 - PubMed
-
- Webb SM, Strasburger CJ, Mo D, et al. Changing patterns of the adult growth hormone deficiency diagnosis documented in a decade-long global surveillance database. J Clin Endocrinol Metab. 2009;94:392–399 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
