

Serpiginous choroiditis and infectious multifocal serpiginoid choroiditis
- PMID: 23541041
- PMCID: PMC3631461
- DOI: 10.1016/j.survophthal.2012.08.008
Serpiginous choroiditis and infectious multifocal serpiginoid choroiditis
Abstract
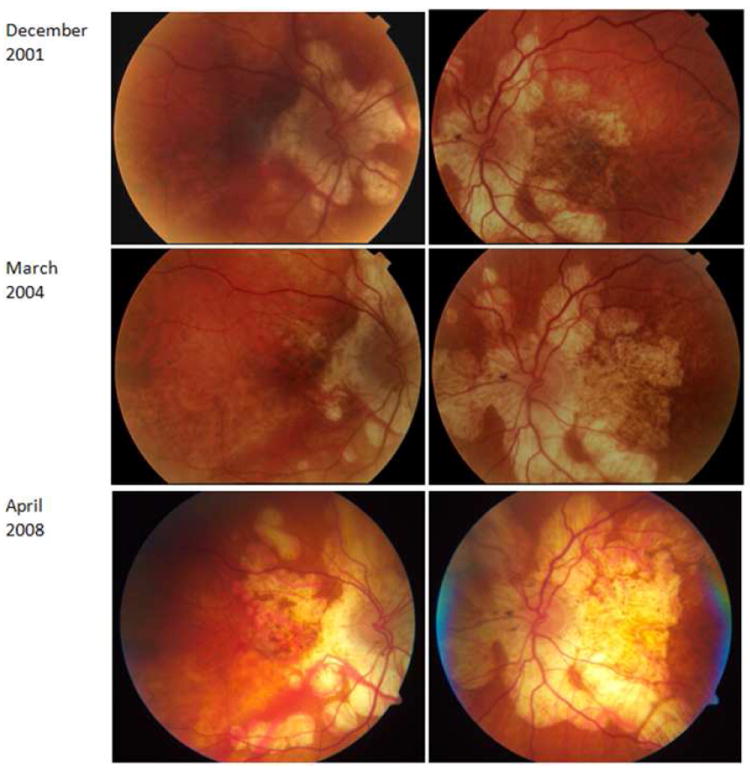
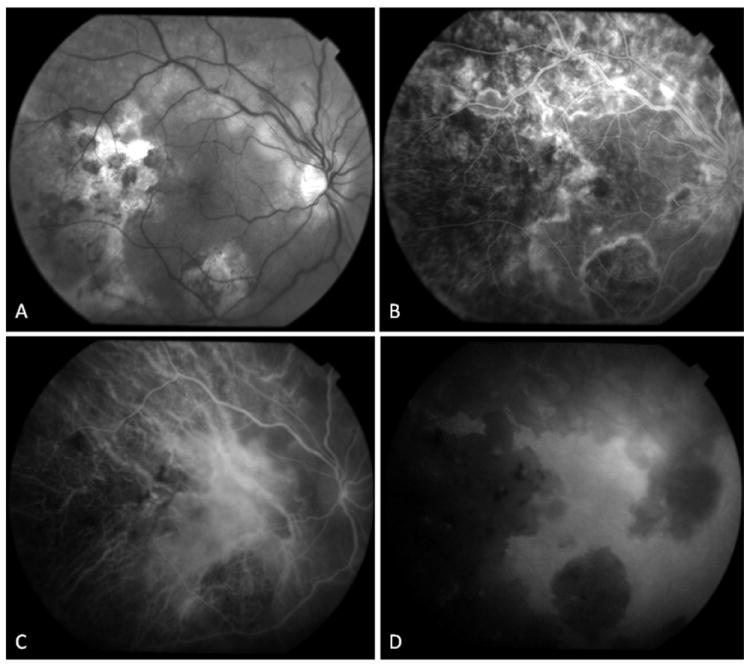
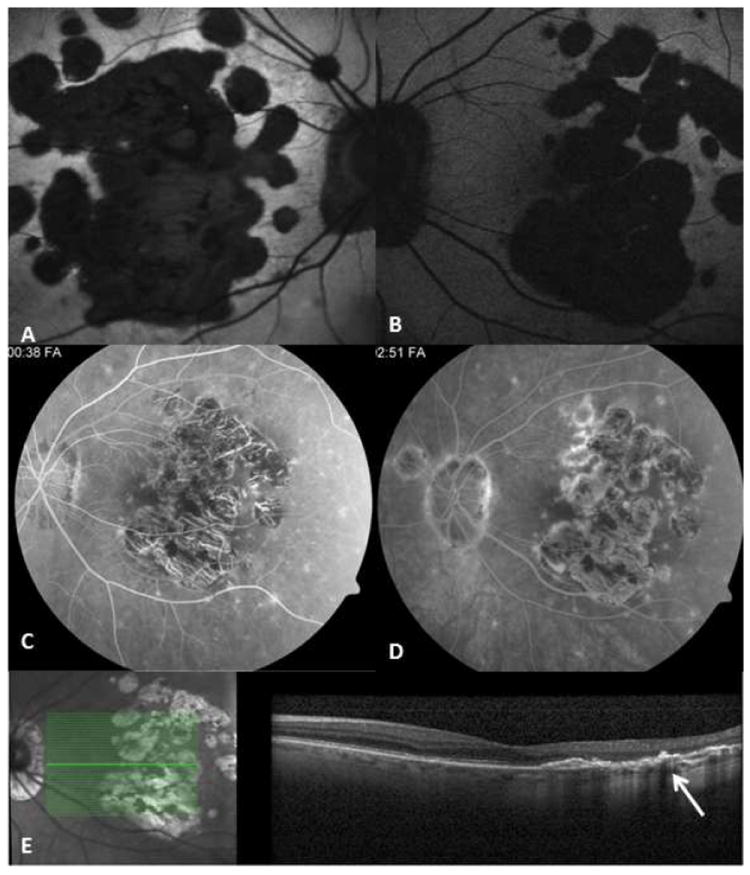
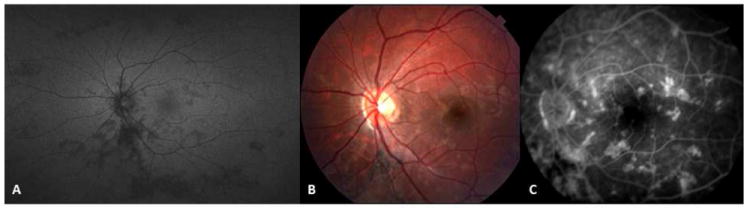
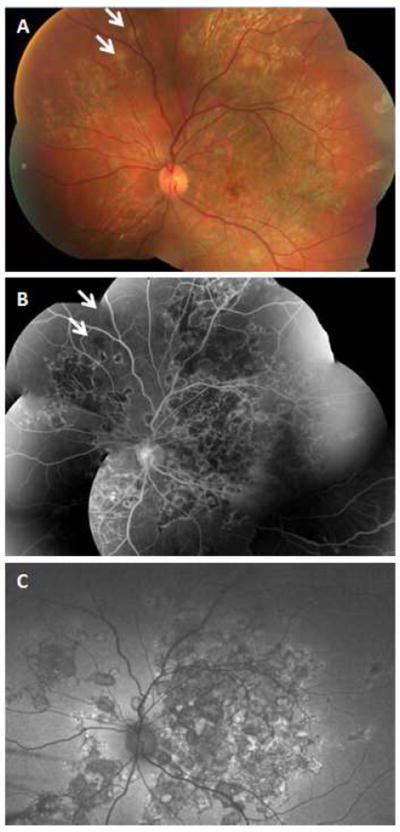
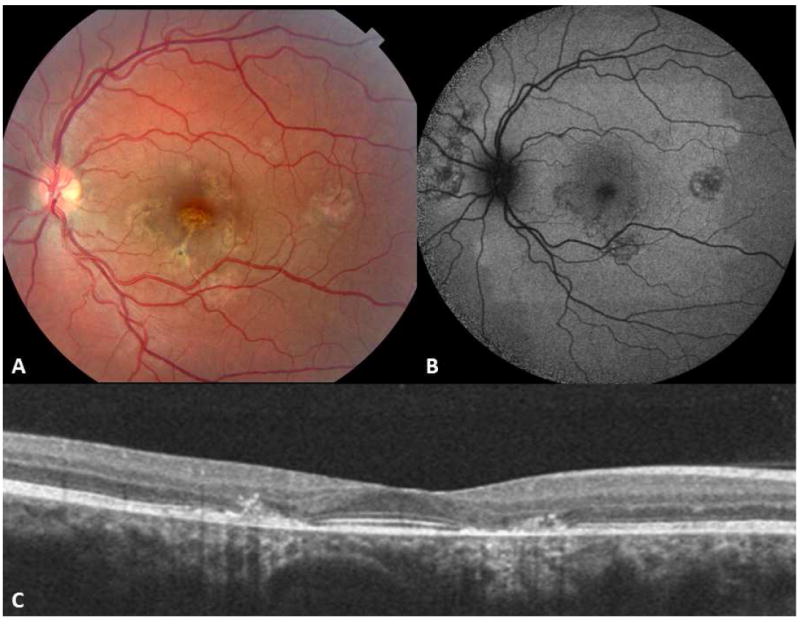
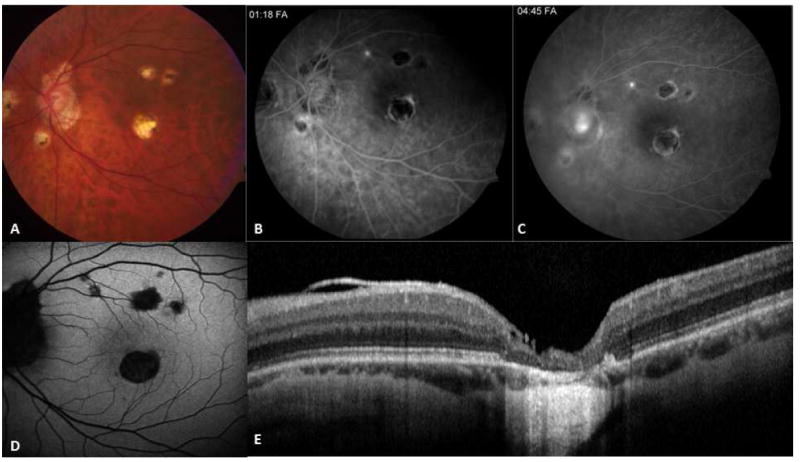
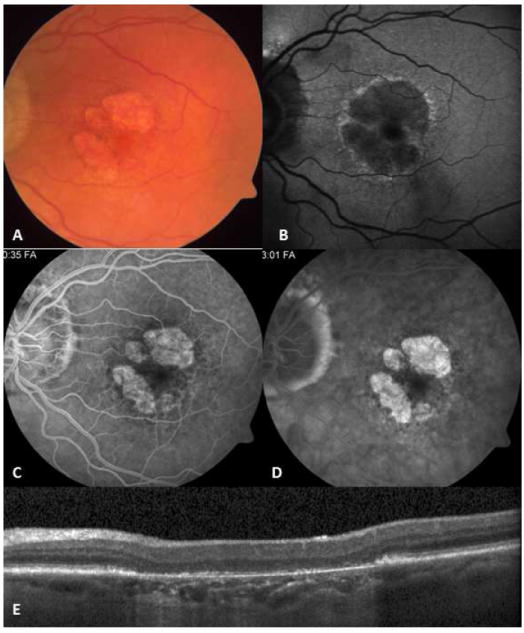
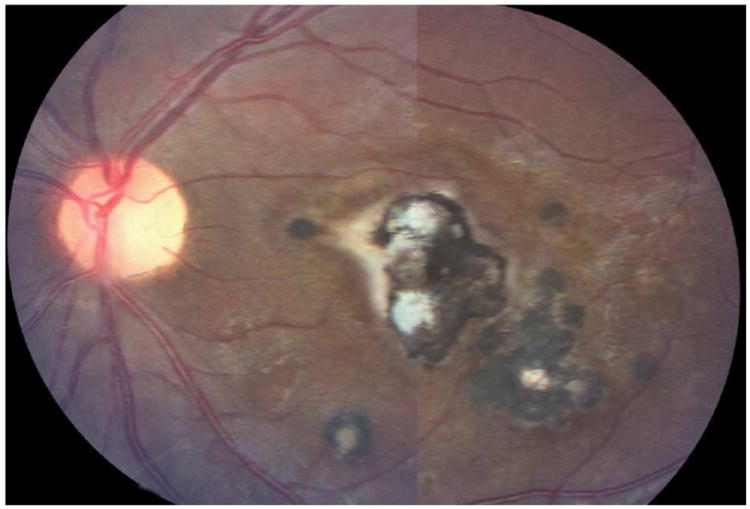
Serpiginous choroiditis (SC) is a posterior uveitis displaying a geographic pattern of choroiditis, extending from the juxtapapillary choroid and intermittently spreading centrifugally. The choroiditis involves the overlying retinal pigment epithelium, and the outer retina. This intraocular inflammation typically involves both eyes in otherwise healthy, middle-aged individuals with no familial or ethnic predilection. Pathogenesis is unclear; based on limited histopathologic studies, however, favorable response to immunosuppressive agents, and the absence of association with systemic or local infectious or noninfectious diseases, an organ-specific autoimmune inflammation seems likely to be the underlying process. Patients, particularly from tuberculosis-endemic regions, may present with fundus changes simulating SC, but show evidence of active tuberculosis and/or the presence of mycobacterial DNA in the aqueous humor. This has been referred to as serpiginous-like choroiditis, but we prefer the description multifocal serpiginoid choroiditis (MSC). We present the distinguishing features of SC and infectious multifocal serpiginoid choroiditis simulating SC. The distinction is crucial to avoid unnecessarily treating SC with antimicrobial agents. Advances in diagnostic and imaging modalities can help differentiate SC from MSC. Novel local and systemic treatment approaches improve the outcome and preserve vision in SC.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- Abrams J, Schlaegel TF., Jr The tuberculin skin test in the diagnosis of tuberculous uveitis. Am J Ophthalmol. 1983;96(3):295–8. - PubMed
-
- Abrez H, Biswas J, Sudharshan S. Clinical profile, treatment, and visual outcome of serpiginous choroiditis. Ocul Immunol Inflamm. 2007;15(4):325–35. - PubMed
-
- Abu el-Asrar AM. Serpiginous (geographical) choroiditis. Int Ophthalmol Clin. 1995;35(2):87–91. - PubMed
-
- Adigüzel U, Sari A, Ozmen C, Oz O. Intravitreal triamcinolone acetonide treatment for serpiginous choroiditis. Ocul Immunol Inflamm. 2006;14(6):375–8. - PubMed
-
- Akpek EK, Baltatzis S, Yang J, Foster CS. Long-term immunosuppressive treatment of serpiginous choroiditis. Ocul Immunol Inflamm. 2001;9(3):147–67. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
