

Impact of baseline heart failure burden on post-implantable cardioverter-defibrillator mortality among medicare beneficiaries
- PMID: 23541973
- PMCID: PMC5587185
- DOI: 10.1016/j.jacc.2013.02.043
Impact of baseline heart failure burden on post-implantable cardioverter-defibrillator mortality among medicare beneficiaries
Abstract
Objectives: This study sought to assess the impact of baseline heart failure (HF) burden on survival with primary implantable cardioverter-defibrillator (ICD) among Medicare recipients.
Background: Survival after primary ICD implantation may differ between trial and Medicare populations.
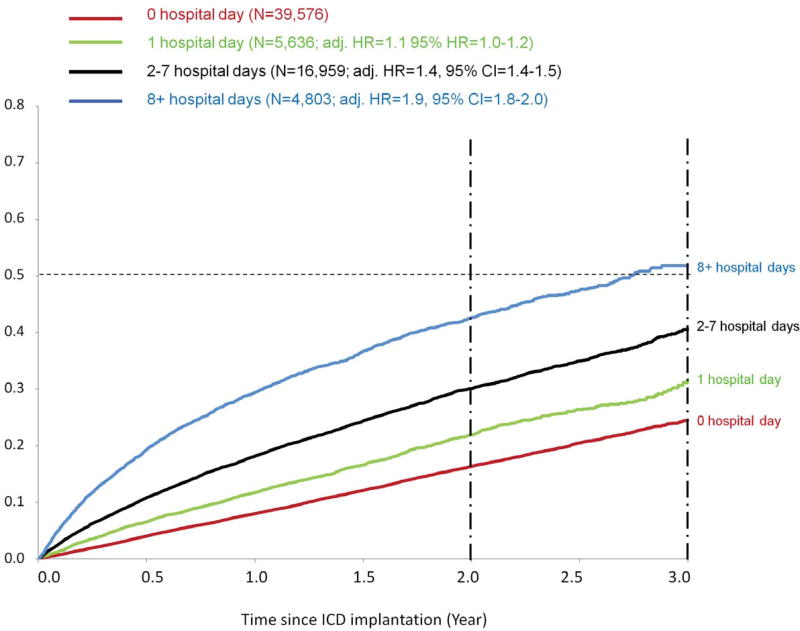
Methods: Linking data from the CMS (Centers for Medicare and Medicaid Services) ICD registry and the Medicare files (2005 to 2009), we identified primary ICD recipients age ≥66 years with ejection fraction ≤35%. Number of previous HF hospitalizations (prev-HF-hosp) and length of hospitalization prior to implantation were used to define HF burden. Crude all-cause mortality was estimated. Adjusted hazard ratios (HR) were derived from Cox models.
Results: Of 66,974 ICD recipients (73% men, 88% white, mean age 75 years), 11,876 died (average follow-up = 1.4 years), with 3-year mortality of 31%. Among patients with no prev-HF-hosp, 3-year mortality was 27% compared with 63% in those with ≥3 prev-HF-hosp (adjusted HR: 1.8). Among patients with same-day implantation, 3-year mortality was 25% compared with 53% in those with >1-week hospitalization days prior to implantation (adjusted HR: 1.9). Mortality at 3-year follow-up among the 31,685 ICD recipients with no prev-HF-hosp and same-day implantation (low HF burden) was similar to that in trials (22%).
Conclusions: Nearly one-third of Medicare ICD recipients died within 3 years, reflecting a population with more advanced age and disease than seen in trial populations for primary prevention ICD. Nearly one-half of Medicare recipients had a low HF burden and had a survival similar to trial ICD recipients. Future research is warranted to understand the effectiveness of primary ICD implantation among Medicare beneficiaries with heavy HF burdens.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures


Comment in
-
Is electricity useful when the pump is failing?: more data urgently needed.J Am Coll Cardiol. 2013 May 28;61(21):2151-2. doi: 10.1016/j.jacc.2013.03.012. Epub 2013 Mar 26. J Am Coll Cardiol. 2013. PMID: 23541963 No abstract available.
References
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
-
- Bristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140–50. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83. - PubMed
-
- CMS National Coverage Determination for ICD. 2005
-
- Fonarow GC, Yancy CW, Hernandez AF, Peterson ED, Spertus JA, Heidenreich PA. Potential impact of optimal implementation of evidence-based heart failure therapies on mortality. Am Heart J. 2011;161:1024–1030. e3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
