

Prevalence and outcomes of cryptococcal antigenemia in HIV-seropositive patients hospitalized for suspected tuberculosis in Uganda
- PMID: 23542636
- PMCID: PMC3779784
- DOI: 10.1097/QAI.0b013e3182926f95
Prevalence and outcomes of cryptococcal antigenemia in HIV-seropositive patients hospitalized for suspected tuberculosis in Uganda
Abstract
Background: Cryptococcal infection occurs in HIV-seropositive patients and is associated with high mortality. However, limited information is available on the prevalence and outcomes of cryptococcal antigenemia among hospitalized HIV-seropositive patients in sub-Saharan Africa.
Objectives: To determine the prevalence of and risk factors for cryptococcal antigenemia among HIV-seropositive patients presenting to Mulago Hospital (Kampala, Uganda) with unexplained cough ≥2 weeks and suspected tuberculosis (TB) and also to determine if antigenemia is associated with an increased mortality.
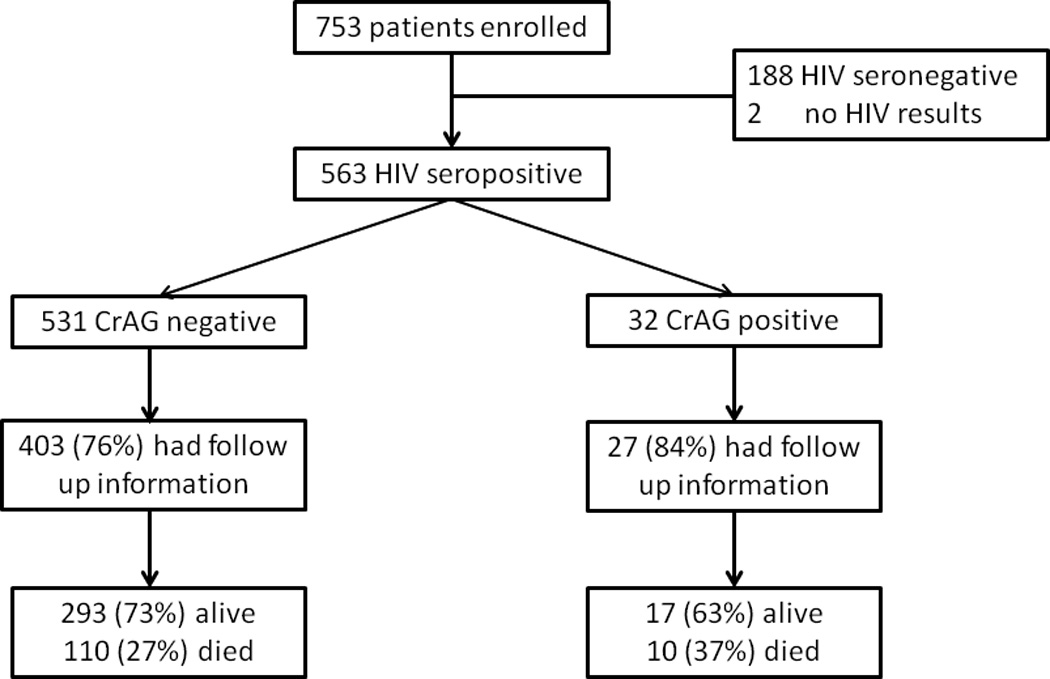
Methods: Between September 2009 and September 2010, we enrolled consecutive HIV-seropositive adults hospitalized at Mulago Hospital with cough ≥2 weeks and suspected TB. Banked serum was tested for cryptococcal antigen. We compared demographic and clinical characteristics, and 2-month mortality in patients with and without cryptococcal antigenemia.
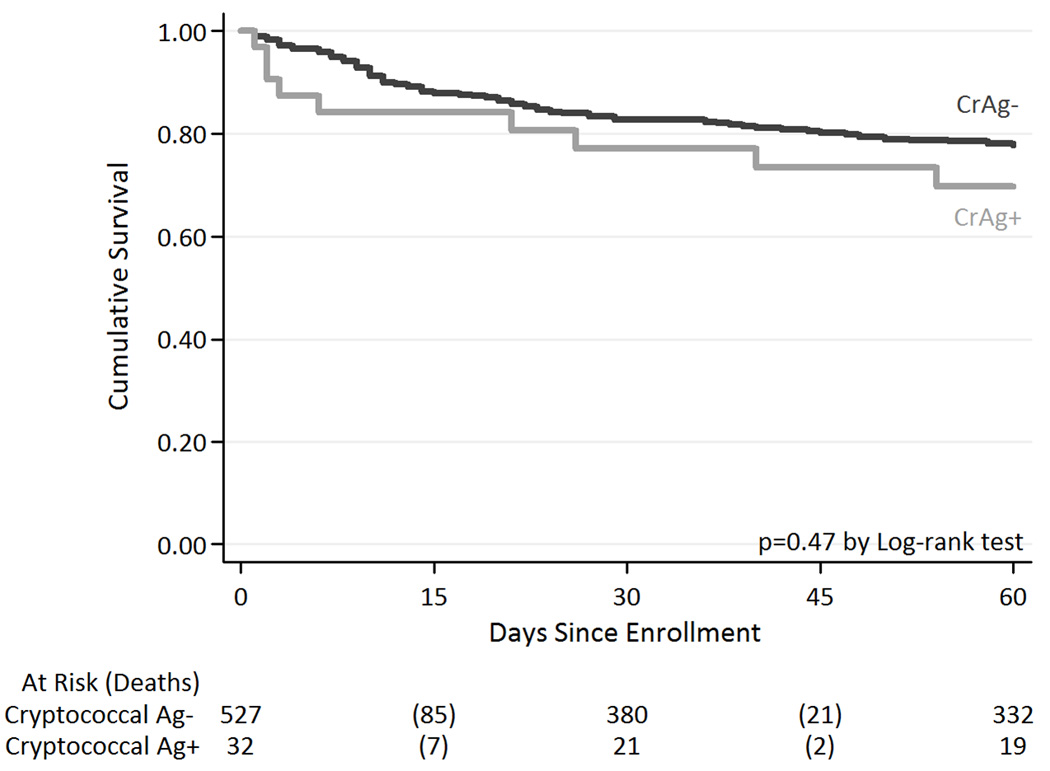
Results: Of 563 HIV-seropositive patients, 32 (5.7%) were cryptococcal antigen (CrAg) positive. None had Cryptococcus neoformans detected on fungal culture of bronchoalveolar lavage fluid (n = 116). CrAg-positive patients had a lower median CD4 count compared with CrAg-negative patients (25 vs. 55 cells/μL, P = 0.02), and a substantial proportion of CrAg-positive patients also had concurrent TB (31%). A positive CrAg test was not associated with increased mortality during the 2-month follow-up period (hazard ratio: 0.99, 95% confidence interval: 0.63 to 1.54, P = 0.95) after adjusting for CD4 count and antiretroviral therapy use at enrollment and/or follow-up.
Conclusions: Occult cryptococcal antigenemia occurs commonly among hospitalized HIV-seropositive patients with suspected TB. CrAg testing should be considered in hospitalized HIV-seropositive patients with CD4 count <50 cells/μL, coupled with longer follow-up to evaluate the diagnostic value of CrAg and therapeutic interventions in patients with asymptomatic cryptococcal antigenemia.
Conflict of interest statement
References
-
- Park BJ, Wannemuehler KA, Marston BJ, Govender N, Pappas PG, Chiller TM. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS. 2009;23:525–530. - PubMed
-
- CDC. Cryptococcosis. 2000
-
- French N, Gray K, Watera C, Nakiyingi J, Lugada E, Moore M. Cryptococcal infection in a cohort of HIV-1-infected Ugandan adults. AIDS. 2002;16:1031–1038. - PubMed
-
- Churchyard GJ, Kleinschmidt I, Corbett EL, Murray J, Smit J, de Cock KM. Factors associated with an increased case-fatality rate in HIV-infected and non-infected South African gold miners with pulmonary tuberculosis. Int J Tuberc Lung Dis. 2000;4:705–712. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
