

Subclinical pretreatment sensory deficits appear to predict the development of pain and numbness in patients with multiple myeloma undergoing chemotherapy
- PMID: 23543296
- PMCID: PMC3669643
- DOI: 10.1007/s00280-013-2152-7
Subclinical pretreatment sensory deficits appear to predict the development of pain and numbness in patients with multiple myeloma undergoing chemotherapy
Abstract
Purpose: Chemotherapy-induced peripheral neuropathy is a major complication in the treatment for cancer, including multiple myeloma (MM). Patients may develop painful and non-painful (e.g., numbness) neuropathy symptoms that impair function and often persist after therapy is terminated. This study tested the hypothesis that baseline subclinical neuropathy, as assessed by sensory thresholds, is related to the development of neuropathy symptoms (e.g., pain and numbness) in patients with MM undergoing treatment with chemotherapy.
Methods: Patients (n = 56) who had undergone two or fewer cycles of induction therapy and who had no evident neuropathy were assessed using quantitative sensory tests to determine multiple-modality sensory thresholds. Patient-reported pain and numbness were assessed through induction therapy (16 weeks) via the MD Anderson Symptom Inventory. A subset of participants (n = 15) continued reporting on their symptoms for an additional 16 weeks ("maintenance phase").
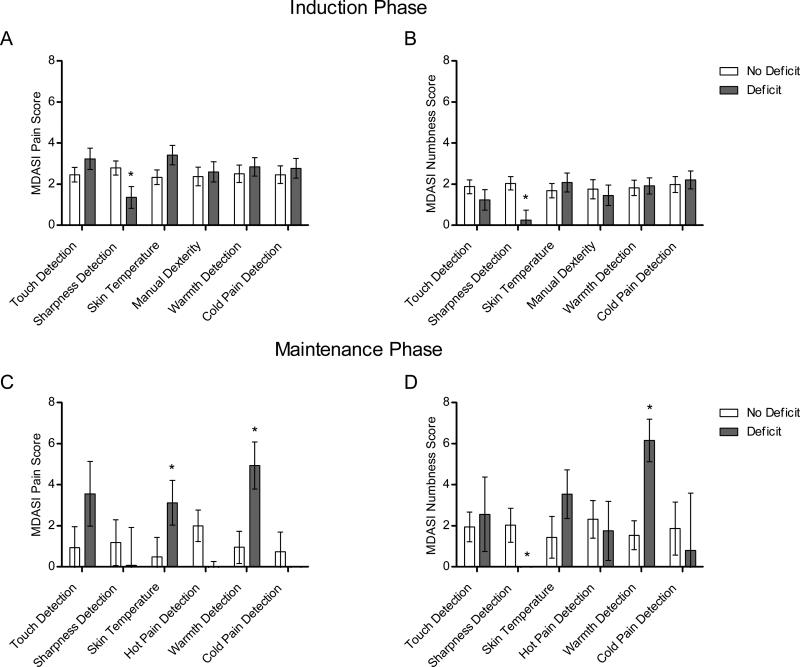
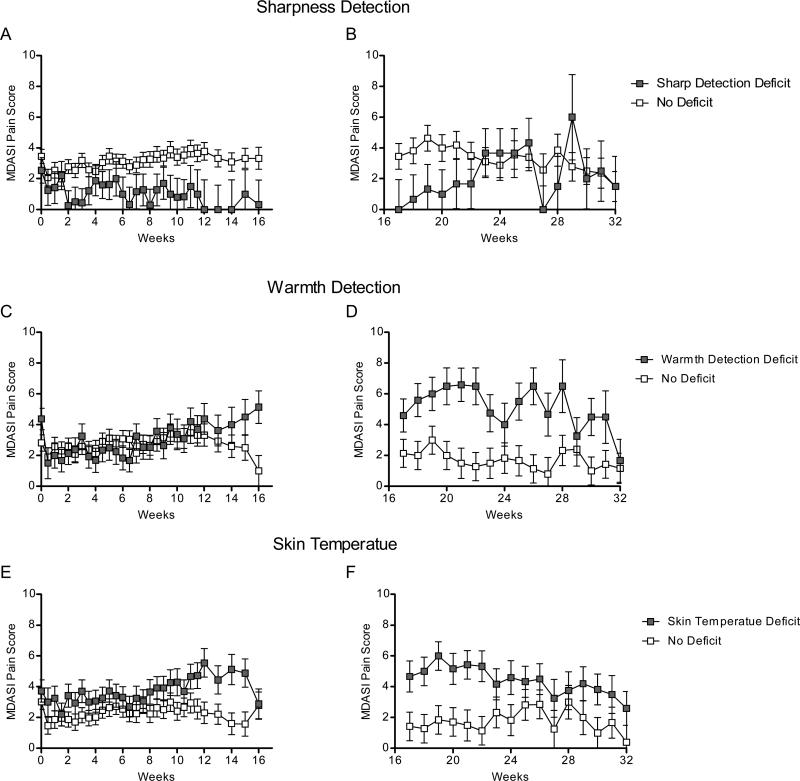
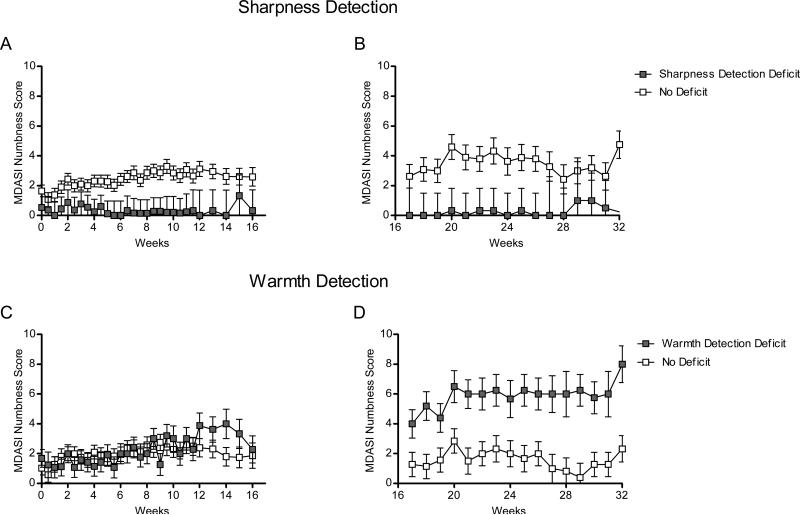
Results: Patients with sharpness detection deficits at baseline (n = 11, 20 % of sample) reported less severe pain and numbness during induction therapy and less numbness during maintenance therapy (P < 0.05). During the maintenance phase, patients with warmth detection deficits (n = 5, 38 % of sample) reported more severe pain and numbness, and those with skin temperature deficits (n = 7, 47 % of maintenance sample) reported more severe pain (P < 0.05). These deficits were related to patient reported difficulty walking, a common symptom of peripheral neuropathy.
Conclusion: Our results suggest that baseline subclinical sensory deficits may be related to a patient's risk for developing chemotherapy-induced peripheral neuropathy.
Figures
References
-
- Aghajanian C, Soignet S, Dizon DS, Pien CS, Adams J, Elliott PJ, Sabbatini P, Miller V, Hensley ML, Pezzulli S, Canales C, Daud A, Spriggs DR. A phase I trial of the novel proteasome inhibitor PS341 in advanced solid tumor malignancies. Clin Cancer Res. 2002;8(8):2505–2511. - PubMed
-
- Jagannath S, Durie BG, Wolf J, Camacho E, Irwin D, Lutzky J, McKinley M, Gabayan E, Mazumder A, Schenkein D, Crowley J. Bortezomib therapy alone and in combination with dexamethasone for previously untreated symptomatic multiple myeloma. Br J Haematol. 2005;129(6):776–783. doi:10.1111/j.1365-2141.2005.05540.x. - PubMed
-
- Loprinzi CL, Reeves BN, Dakhil SR, Sloan JA, Wolf SL, Burger KN, Kamal A, Le-Lindqwister NA, Soori GS, Jaslowski AJ, Novotny PJ, Lachance DH. Natural history of paclitaxel-associated acute pain syndrome: prospective cohort study NCCTG N08C1. J Clin Oncol. 2011;29(11):1472–1478. doi:JCO.2010.33.0308 [pii] 10.1200/JCO.2010.33.0308. - PMC - PubMed
-
- Tofthagen C. Patient perceptions associated with chemotherapy-induced peripheral neuropathy. Clin J Oncol Nurs. 2010;14(3):E22–28. doi:758N375251807W57 [pii] 10.1188/10.CJON.E22-E28. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
