

Relevance of the Core 70 and IL-28B polymorphism and response-guided therapy of peginterferon alfa-2a ± ribavirin for chronic hepatitis C of Genotype 1b: a multicenter randomized trial, ReGIT-J study
- PMID: 23543311
- PMCID: PMC3953545
- DOI: 10.1007/s00535-013-0785-2
Relevance of the Core 70 and IL-28B polymorphism and response-guided therapy of peginterferon alfa-2a ± ribavirin for chronic hepatitis C of Genotype 1b: a multicenter randomized trial, ReGIT-J study
Abstract
Background: We conducted a multicenter randomized clinical trial to determine the optimal treatment strategy against chronic hepatitis C virus (HCV) with genotype 1b and a high viral load (G1b/high).
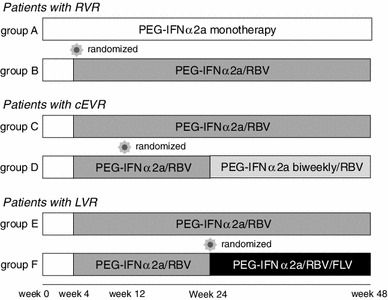
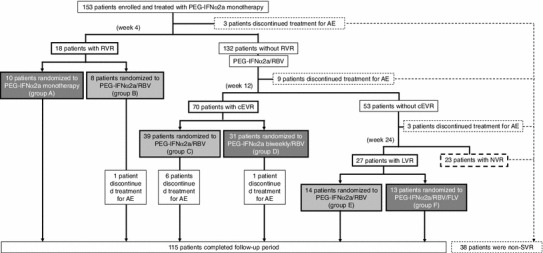
Methods: The study subjects included 153 patients with G1b/high. Patients were initially treated with PEG-IFNα-2a alone and then randomly assigned to receive different treatment regimens. Ribavirin (RBV) was administered to all patients with HCV RNA at week 4. Patients negative for HCV RNA at week 4 were randomly assigned to receive PEG-IFNα-2a (group A) or PEG-IFNα-2a/RBV (group B). Patients who showed HCV RNA at week 4 but were negative at week 12 were randomly assigned to receive weekly PEG-IFNα-2a (group C) or biweekly therapy (group D). Patients who showed HCV RNA at week 12 but were negative at week 24 were randomly assigned to receive PEG-IFNα-2a/RBV (group E) or PEG-IFNα-2a/RBV/fluvastatin (group F).
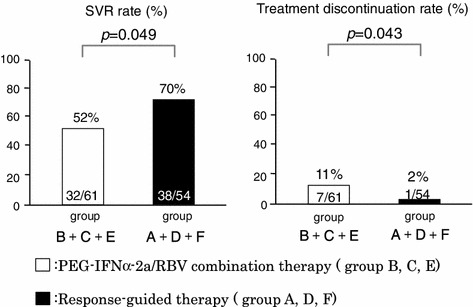
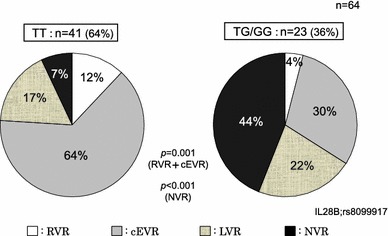
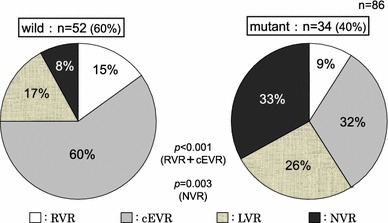
Results: Overall, the rate of sustained virological response (SVR) was 46 % (70/153). The total SVR rate in the group (A, D, and F) of response-guided therapy was significantly higher than that in the group (B, C, and E) of conventional therapy [70 % (38/54) versus 52 % (32/61), p = 0.049]. Although IL28-B polymorphism and Core 70 mutation were significantly associated with efficacy, patients with rapid virological response (RVR) and complete early virological response (cEVR) achieved high SVR rates regardless of their status of IL-28B polymorphism and Core 70 mutation.
Conclusion: In addition to knowing the IL-28B polymorphism and Core 70 mutation status, understanding the likelihood of virological response during treatment is critical in determining the appropriate treatment strategy.
Figures
References
-
- Kuboki M, Iino S, Okuno T, Omata M, et al. Peginterferon a-2a (40 KD) plus ribavirin for the treatment of chronic hepatitis C in Japanese patients. J Gastroenterol Hepatol. 2007;22:645–652. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
