

Clinical characteristics of intraspinal facet cysts following microsurgical bilateral decompression via a unilateral approach for treatment of degenerative lumbar disease
- PMID: 23543390
- PMCID: PMC3731472
- DOI: 10.1007/s00586-013-2763-z
Clinical characteristics of intraspinal facet cysts following microsurgical bilateral decompression via a unilateral approach for treatment of degenerative lumbar disease
Abstract
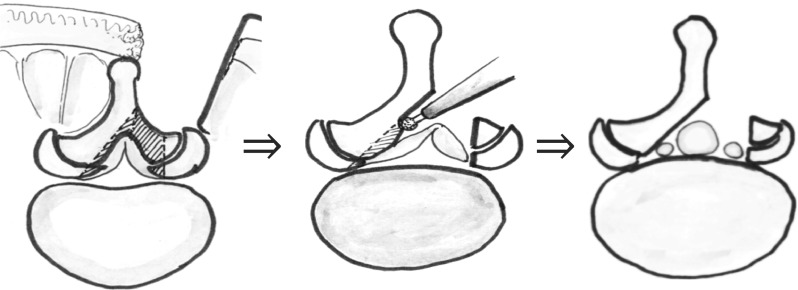
Purpose: Primary intraspinal facet cysts in the lumbar spine are uncommon, but it is unclear whether cyst incidence increases following decompression surgery and if these cysts negatively impact clinical outcome. We examined the prevalence, clinical characteristics, and the risk factors associated with intraspinal facet cysts after microsurgical bilateral decompression via a unilateral approach (MBDU).
Methods: We studied 230 patients treated using MBDU for lumbar degenerative disease (133 men and 97 women; mean age 70.3 years). Clinical status, as assessed by the Japanese Orthopedic Association (JOA) score and findings on X-ray and magnetic resonance images, was evaluated prior to surgery and at both 3 months and 1 year after surgery. The prevalence of intraspinal facet cysts was determined and preoperative risk factors were defined by comparing presurgical findings with clinical outcomes.
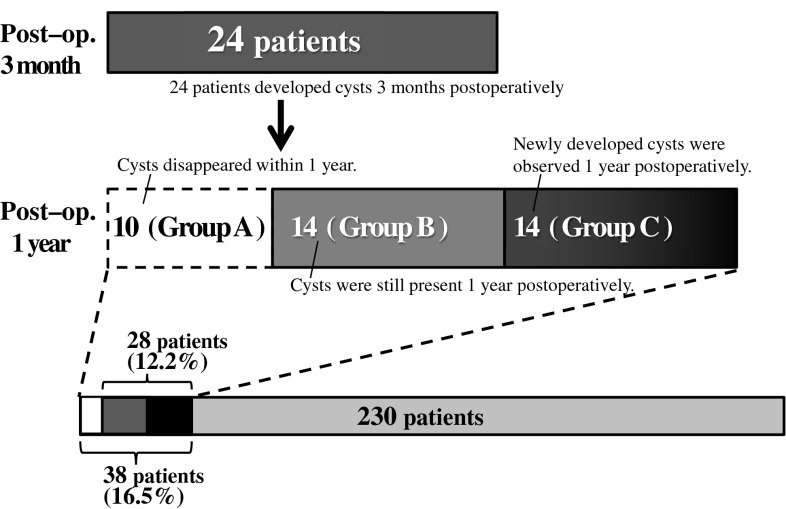
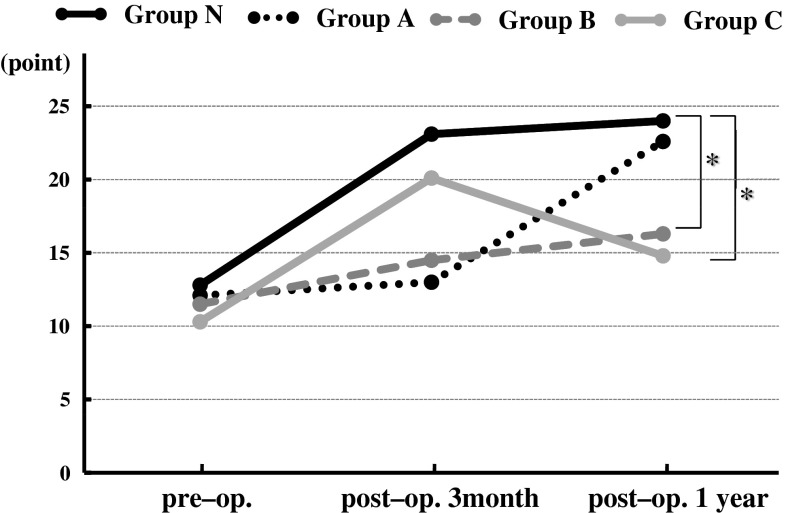
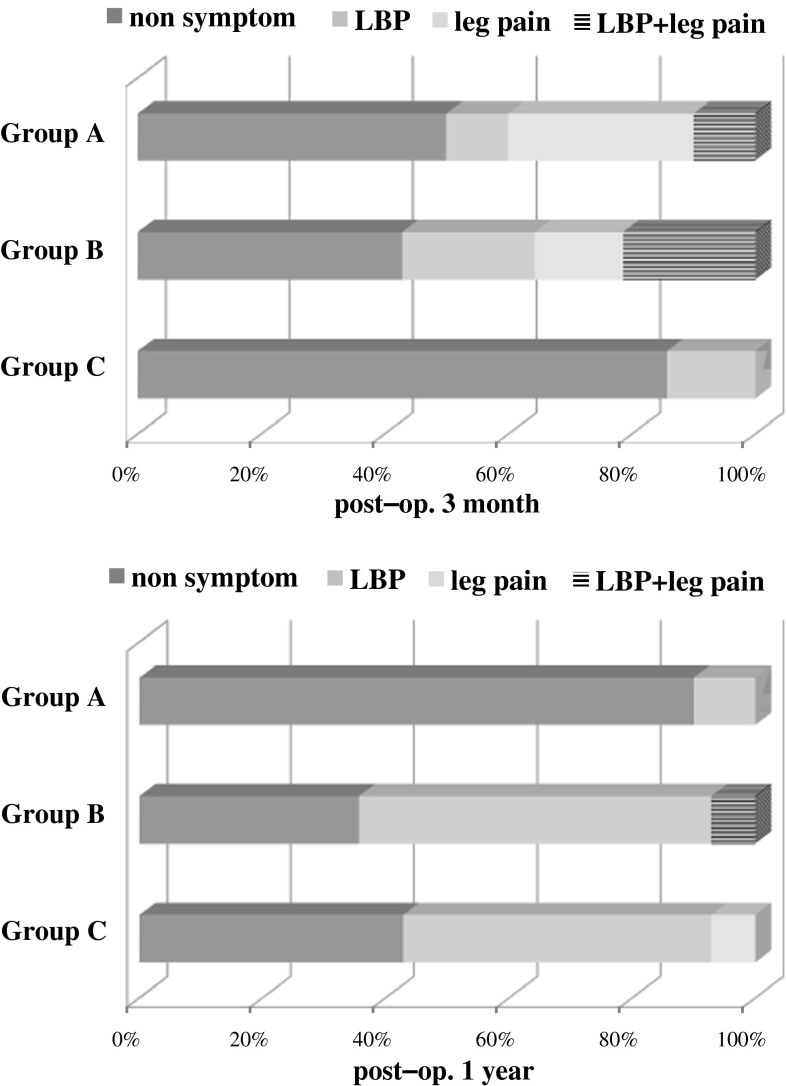
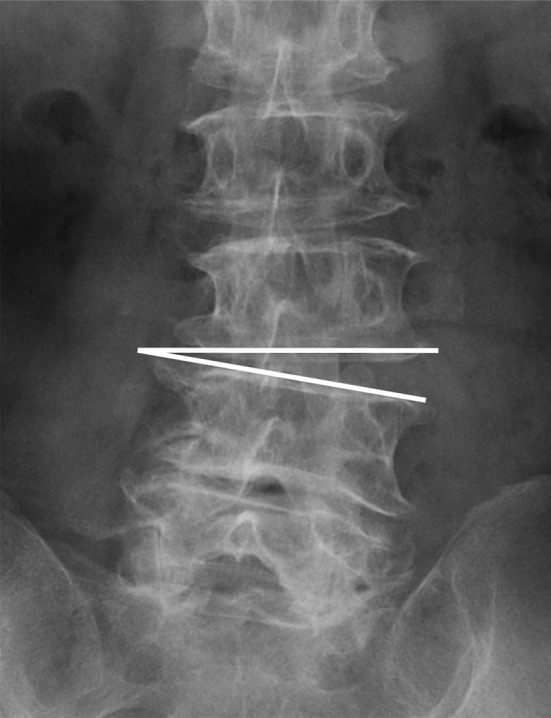
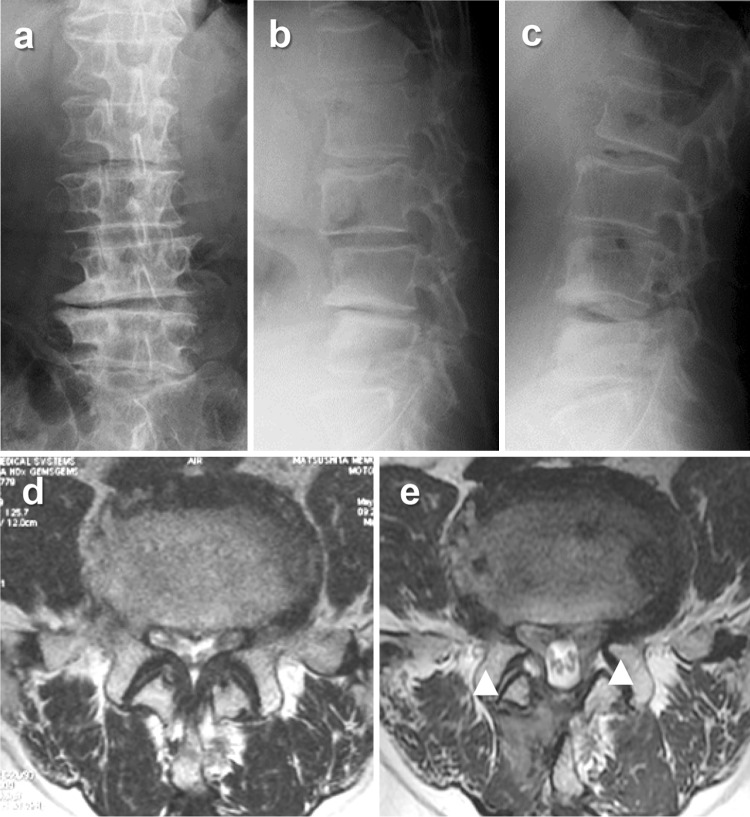
Results: Thirty-eight patients (16.5%) developed intraspinal facet cysts within 1 year postoperatively, and 24 exhibited cysts within 3 months. In 10 patients, the cysts resolved spontaneously 1 year postoperatively. In total, 28 patients (12.2%) had facet cysts 1 year postoperatively. The mean JOA score of patients with cysts 1 year postoperatively was significantly lower than that of patients without cysts. This poor clinical outcome resulted from low back pain that was not improved by conservative treatment. Most cases with spontaneous cyst disappearance were symptom-free 1 year later. The preoperative risk factors for postoperative intraspinal facet cyst formation were instability (OR 2.47, P = 0.26), scoliotic disc wedging (OR 2.23, P = 0.048), and sagittal imbalance (OR 2.22, P = 0.045).
Conclusions: Postoperative intraspinal facet cyst formation is a common cause of poor clinical outcome in patients treated using MBDU.
Figures
References
-
- McCulloch JA, Young PA. Essentials of spinal microsurgery. Philadelphia: Lippincott-Raven; 1998.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
