

Communication skills training for healthcare professionals working with people who have cancer
- PMID: 23543521
- PMCID: PMC6457800
- DOI: 10.1002/14651858.CD003751.pub3
Communication skills training for healthcare professionals working with people who have cancer
Update in
-
Communication skills training for healthcare professionals working with people who have cancer.Cochrane Database Syst Rev. 2018 Jul 24;7(7):CD003751. doi: 10.1002/14651858.CD003751.pub4. Cochrane Database Syst Rev. 2018. PMID: 30039853 Free PMC article.
Abstract
Background: This is an updated version of a review that was originally published in the Cochrane Database of Systematic Reviews in 2004, Issue 2. People with cancer, their families and carers have a high prevalence of psychological stress which may be minimised by effective communication and support from their attending healthcare professionals (HCPs). Research suggests communication skills do not reliably improve with experience, therefore, considerable effort is dedicated to courses that may improve communication skills for HCPs involved in cancer care. A variety of communication skills training (CST) courses have been proposed and are in practice. We conducted this review to determine whether CST works and which types of CST, if any, are the most effective.
Objectives: To assess whether CST is effective in improving the communication skills of HCPs involved in cancer care, and in improving patient health status and satisfaction.
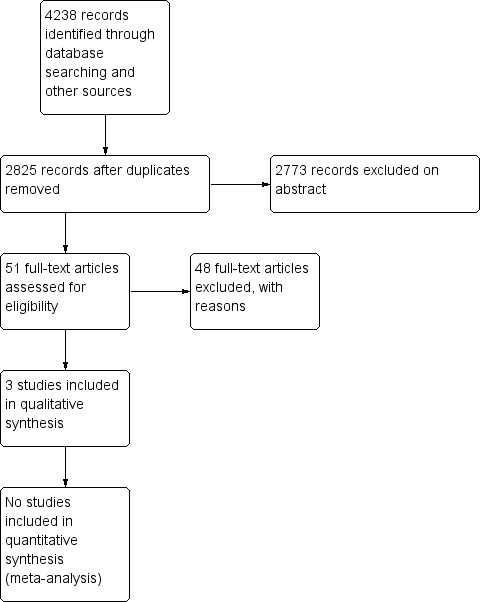
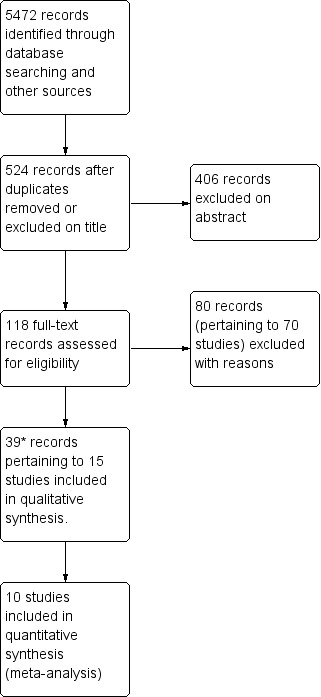
Search methods: We searched the following electronic databases: Cochrane Central Register of Controlled Trials (CENTRAL) Issue 2, 2012, MEDLINE, EMBASE, PsycInfo and CINAHL to February 2012. The original search was conducted in November 2001. In addition, we handsearched the reference lists of relevant articles and relevant conference proceedings for additional studies.
Selection criteria: The original review was a narrative review that included randomised controlled trials (RCTs) and controlled before-and-after studies. In this updated version, we limited our criteria to RCTs evaluating 'CST' compared with 'no CST' or other CST in HCPs working in cancer care. Primary outcomes were changes in HCP communication skills measured in interactions with real and/or simulated patients with cancer, using objective scales. We excluded studies whose focus was communication skills in encounters related to informed consent for research.
Data collection and analysis: Two review authors independently assessed trials and extracted data to a pre-designed data collection form. We pooled data using the random-effects model and, for continuous data, we used standardised mean differences (SMDs).
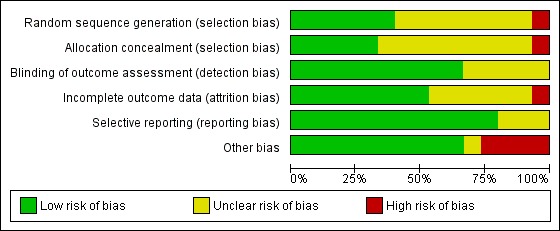
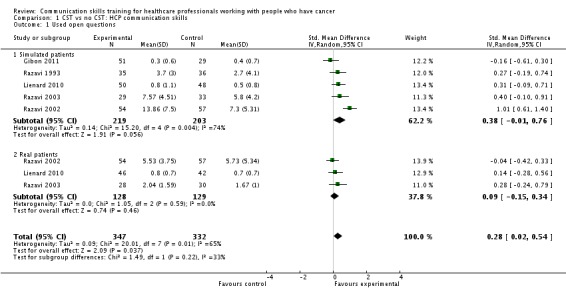
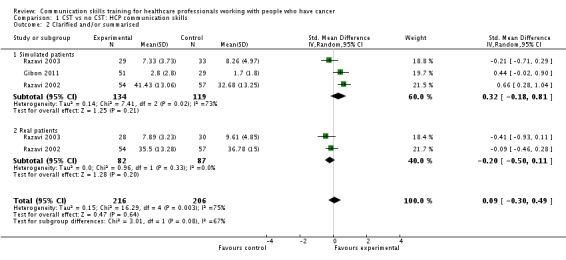
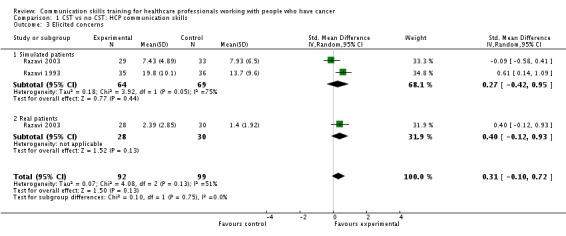
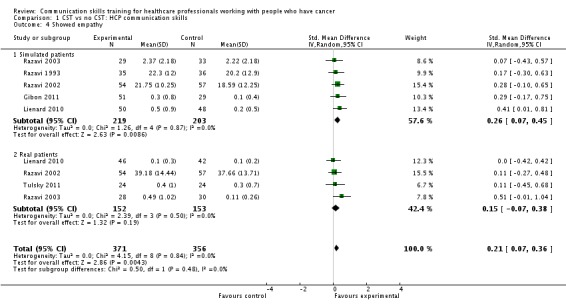
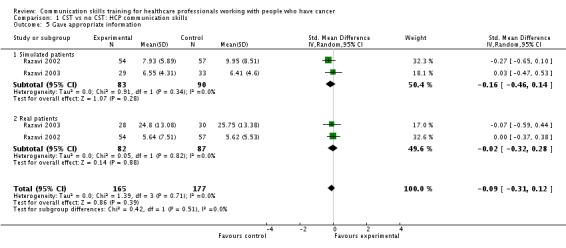
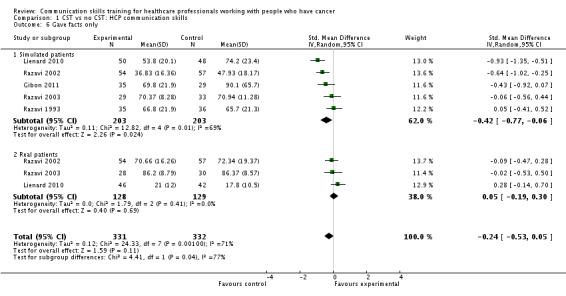
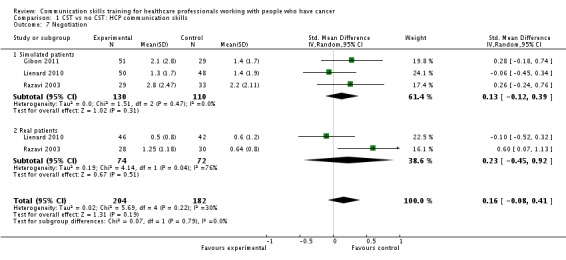
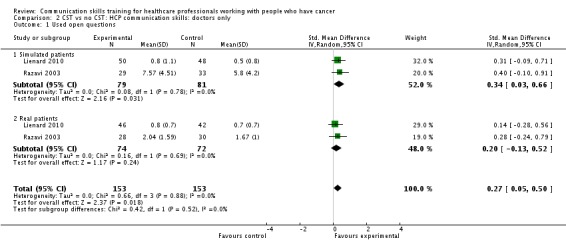
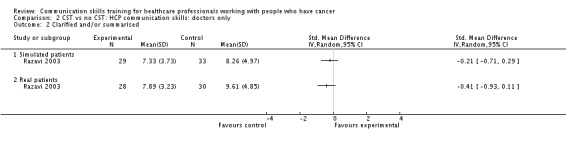
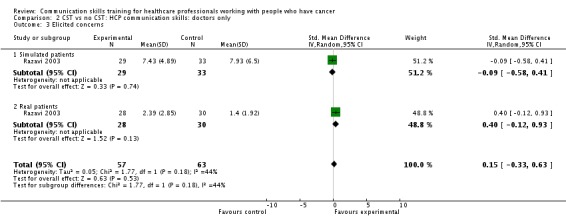
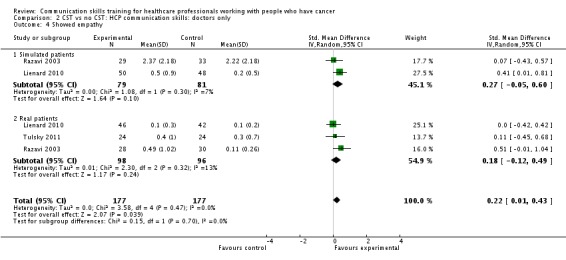
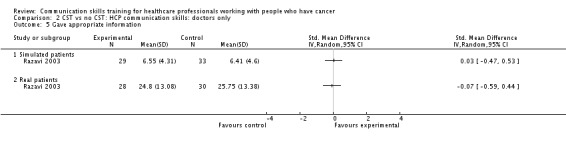
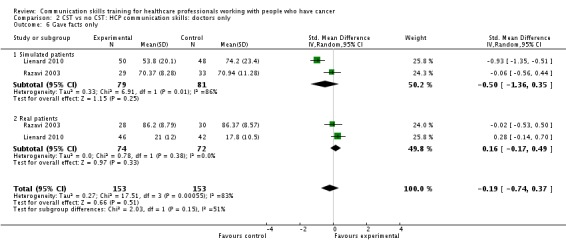
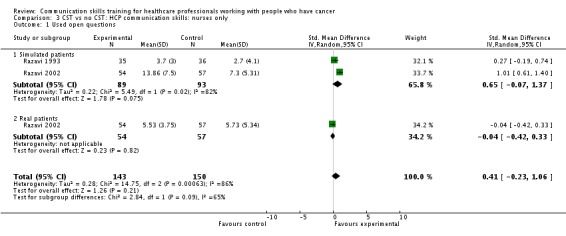
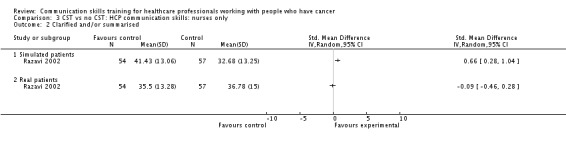
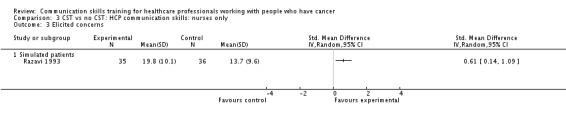
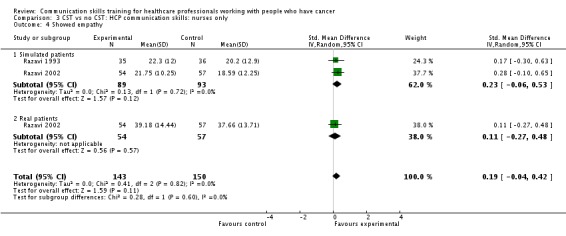
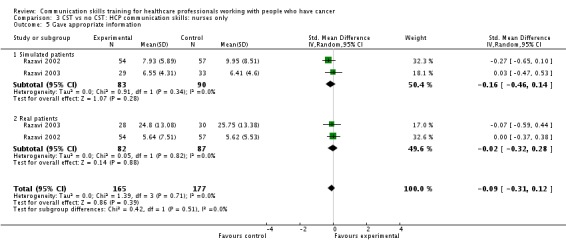
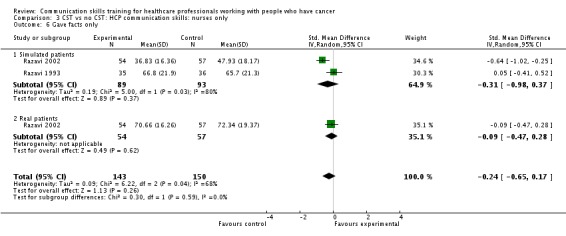
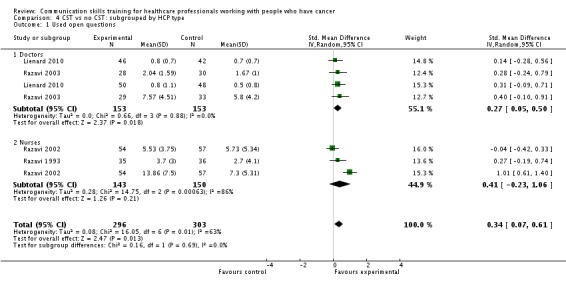
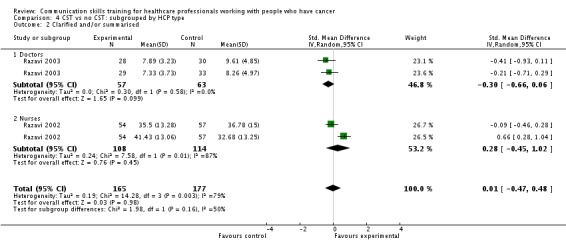
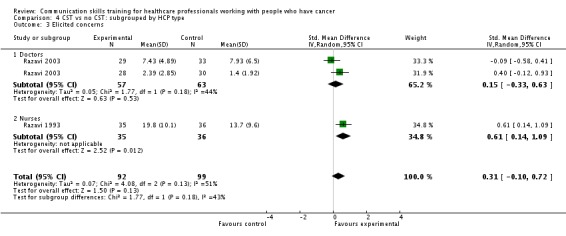
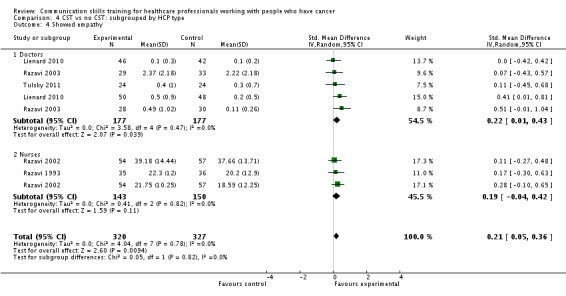
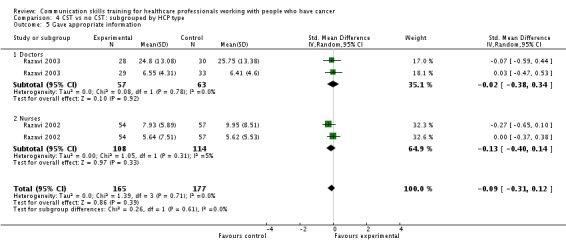
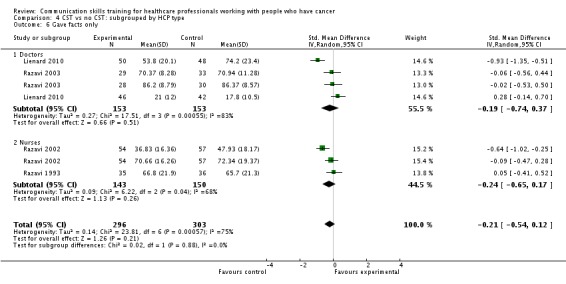
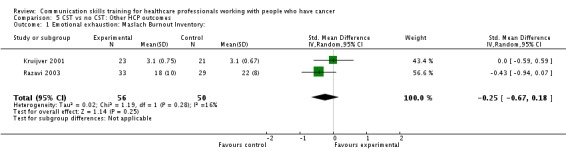
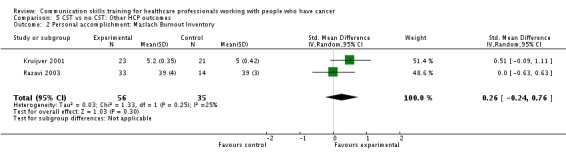
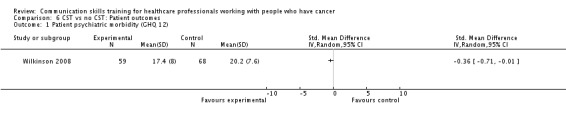
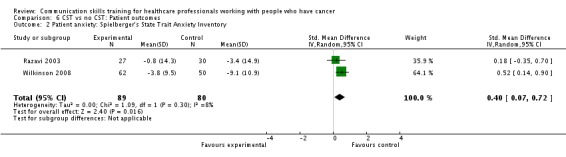
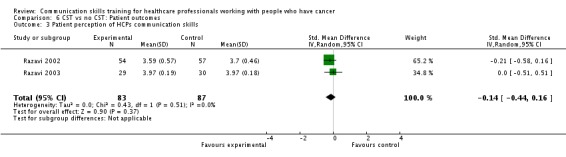
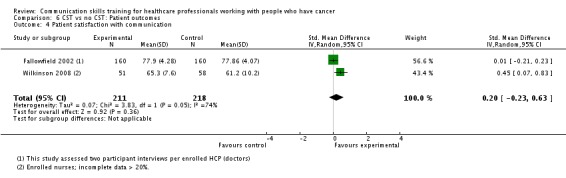
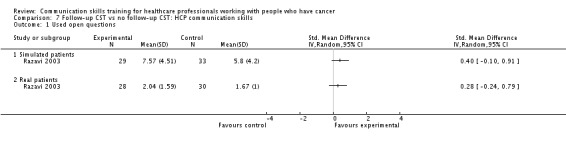
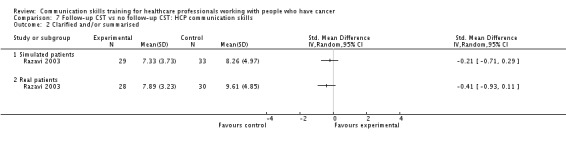
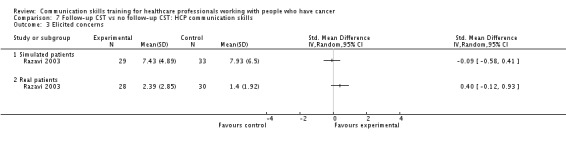
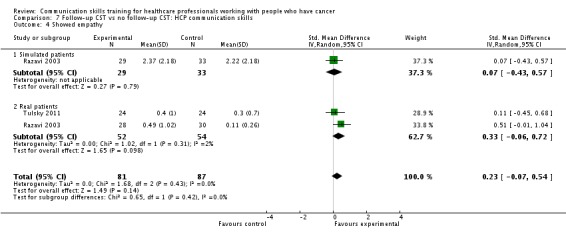
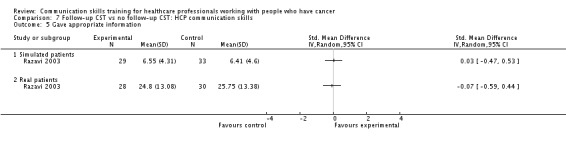
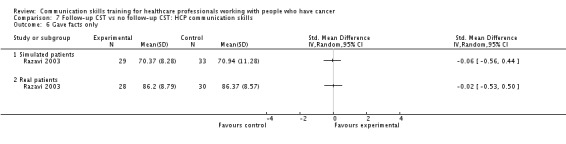
Main results: We included 15 RCTs (42 records), conducted mainly in outpatient settings. Eleven studies compared CST with no CST intervention, three studies compared the effect of a follow-up CST intervention after initial CST training, and one study compared two types of CST. The types of CST courses evaluated in these trials were diverse. Study participants included oncologists (six studies), residents (one study) other doctors (one study), nurses (six studies) and a mixed team of HCPs (one study). Overall, 1147 HCPs participated (536 doctors, 522 nurses and 80 mixed HCPs).Ten studies contributed data to the meta-analyses. HCPs in the CST group were statistically significantly more likely to use open questions in the post-intervention interviews than the control group (five studies, 679 participant interviews; P = 0.04, I² = 65%) and more likely to show empathy towards patients (six studies, 727 participant interviews; P = 0.004, I² = 0%); we considered this evidence to be of moderate and high quality, respectively. Doctors and nurses did not perform statistically significantly differently for any HCP outcomes.There were no statistically significant differences in the other HCP communication skills except for the subgroup of participant interviews with simulated patients, where the intervention group was significantly less likely to present 'facts only' compared with the control group (four studies, 344 participant interviews; P = 0.01, I² = 70%).There were no significant differences between the groups with regard to outcomes assessing HCP 'burnout', patient satisfaction or patient perception of the HCPs communication skills. Patients in the control group experienced a greater reduction in mean anxiety scores in a meta-analyses of two studies (169 participant interviews; P = 0.02; I² = 8%); we considered this evidence to be of a very low quality.
Authors' conclusions: Various CST courses appear to be effective in improving some types of HCP communication skills related to information gathering and supportive skills. We were unable to determine whether the effects of CST are sustained over time, whether consolidation sessions are necessary, and which types of CST programs are most likely to work. We found no evidence to support a beneficial effect of CST on HCP 'burnout', patients' mental or physical health, and patient satisfaction.
Conflict of interest statement
None.
Figures
Update of
-
Communication skills training for health care professionals working with cancer patients, their families and/or carers.Cochrane Database Syst Rev. 2004;(2):CD003751. doi: 10.1002/14651858.CD003751.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2013 Mar 28;(3):CD003751. doi: 10.1002/14651858.CD003751.pub3. PMID: 15106217 Updated.
References
References to studies included in this review
-
- Butow P, Cockburn J, Girgis A, Bowman D, Schofield P, D'Este C, et al. Increasing oncologists' skills in eliciting and responding to emotional cues: evaluation of a communication skills training program. Psycho‐Oncology 2008;17(3):209‐18. - PubMed
- Girgis A, Cockburn J, Butow P, Bowman D, Schofield P, Stojanovski E, et al. Improving patient emotional functioning and psychological morbidity: Evaluation of a consultation skills training program for oncologists. Patient Education and Counseling 2009;77(3):456‐62. - PubMed
-
- Fallowfield L, Jenkins V, Farewell V, Saul J, Duffy A, Eves R. Efficacy of a Cancer Research UK communication skills training model for oncologists: a randomised controlled study. Lancet 2002;359(9307):650‐6. - PubMed
- Fallowfield L, Jenkins V, Farewell V, Solis TI. Enduring impact of communication skills training: results of a 12‐month follow‐up. British Journal of Cancer 2003;89:1445‐9. - PMC - PubMed
- Jenkins V, Fallowfield L. Can communication skills training alter physicians' beliefs and behavior in clinics?. Journal of Clinical Oncology 2002;20:765‐9. - PubMed
- Shilling V, Jenkins V, Fallowfield L. Factors affecting patient and clinician satisfaction with the clinical consultation: can communication skills training for clinicians improve satisfaction?. Psycho‐Oncology 2003;12:599‐611. - PubMed
-
- Fujimori MS. Effect of communication skills training program for oncologists based on the patient preferences for communicating bad news: A randomized control trial. Psycho‐Oncology Conference: 13th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Antalya Turkey. Conference Start: 20111016 Conference End: 20111020. 2011:Conference Publication:[var.pagings].
-
- Gibon A‐SM. Is it possible to improve radiotherapy team communication skills? A randomized study assessing the efficacy of a training program in the context of an encounter with a simulated anxious patient called Mrs Leblanc. Psycho‐Oncology. 2011; Vol. 13th World Congress of the International Psycho‐Oncology Society 16/01/2011 ‐20/01/2011, Antalya, Turkey:[Var. pagings].
-
- Goeltz TW. The transition from curative to palliative care in oncology‐a special challenge requires special communication skills training. Evaluation of a specific and individualized training concept‐a RCT. Psycho‐Oncology Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625. 2009:Conference Publication:[var.pagings].
- Goelz T, Wuensch A, Stubenrauch S, Ihorst G, Figueiredo M, Bertz H, et al. Specific training program improves oncologists' palliative care communication skills in a randomized controlled trial. Journal of Clinical Oncology 2011;29(25):3402‐7. - PubMed
- Goelz TW. Psycho‐Oncology; Conference(var.pagings). Conference Publication, 2010; Vol. 19(Suppl 2):S1‐S313.
References to studies excluded from this review
-
- Archer M, Daniel R, Riley J, Wynburne J. Empowering people with cancer. Expert Review of Anticancer Therapy 2004;4(3 Suppl. 1):S51‐7. - PubMed
-
- Ades T, Gansler T, Eyre H. Communicating with patients about quality of life issues. CA: A Cancer Journal for Clinicians 2001;51(4):211‐2. - PubMed
-
- Alexander SC, Keitz SA, Sloane R, Tulsky JA. A controlled trial of a short course to improve residents' communication with patients at the end of life. Academic Medicine 2006;81(11):1008‐12. - PubMed
-
- Anderson JL. Evaluation of a practical approach to teaching about communication with terminal cancer patients. Medical Education 1982;16(4):202‐7. - PubMed
-
- Andrew M. The dilemmas of experiential teaching: toward an interpretive approach. Journal of Continuing Education in Nursing 1998;29(2):73‐8. - PubMed
Additional references
-
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ‐C30: A Quality‐of‐Life Instrument for Use in International Clinical Trials in Oncology. Journal of the National Cancer Institute 1993;85(5):365‐76. - PubMed
-
- ACGME (Accreditiation Council for Graduate Medical Education). Common Program Requirements. ACGME 2009. Available from: http://www.acgme.org/acWebsite/dutyHours/dh_dutyhoursCommonPR07012007.pdf.
-
- Adamo G. Simulated and standardized patients in OSCEs: achievements and challenges 1992‐2003. Medical Teacher 2003;25(3):262‐70. - PubMed
-
- Alvarez MP, Agra Y. Systematic review of educational interventions in palliative care for primary care physicians. Palliative Medicine 2006;20(7):673‐83. - PubMed
-
- Ashworth CD, Williamson P, Montano D. A scale to measure physician beliefs about psychosocial aspects of patient care. Social Science & Medicine 1984;19(11):1235‐8. - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous