

Uric acid and chronic kidney disease: which is chasing which?
- PMID: 23543594
- PMCID: PMC4318947
- DOI: 10.1093/ndt/gft029
Uric acid and chronic kidney disease: which is chasing which?
Abstract
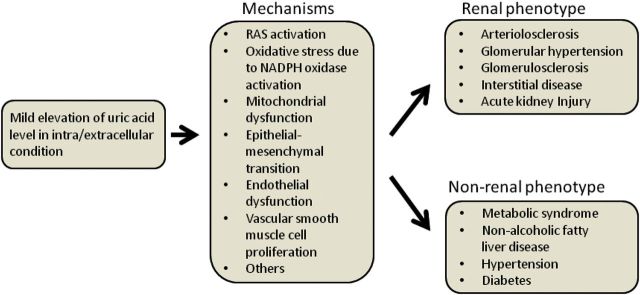
Serum uric acid is commonly elevated in subjects with chronic kidney disease (CKD), but was historically viewed as an issue of limited interest. Recently, uric acid has been resurrected as a potential contributory risk factor in the development and progression of CKD. Most studies documented that an elevated serum uric acid level independently predicts the development of CKD. Raising the uric acid level in rats can induce glomerular hypertension and renal disease as noted by the development of arteriolosclerosis, glomerular injury and tubulointerstitial fibrosis. Pilot studies suggest that lowering plasma uric acid concentrations may slow the progression of renal disease in subjects with CKD. While further clinical trials are necessary, uric acid is emerging as a potentially modifiable risk factor for CKD. Gout was considered a cause of CKD in the mid-nineteenth century, and, prior to the availability of therapies to lower the uric acid level, the development of end-stage renal disease was common in gouty patients. In their large series of gouty subjects Talbott and Terplan found that nearly 100% had variable degrees of CKD at autopsy (arteriolosclerosis, glomerulosclerosis and interstitial fibrosis). Additional studies showed that during life impaired renal function occurred in half of these subjects. As many of these subjects had urate crystals in their tubules and interstitium, especially in the outer renal medulla, the disease became known as gouty nephropathy. The identity of this condition fell in question as the presence of these crystals may occur in subjects without renal disease; furthermore, the focal location of the crystals could not explain the diffuse renal scarring present. In addition, many subjects with gout also had coexistent conditions such as hypertension and vascular disease, leading some experts to suggest that the renal injury in gout was secondary to these latter conditions rather than to uric acid per se. Indeed, gout was removed from the textbooks as a cause of CKD, and the common association of hyperuricemia with CKD was solely attributed to the retention of serum uric acid that is known to occur as the glomerular filtration rate falls. Renewed interest in uric acid as a cause of CKD occurred when it was realized that invalid assumptions had been made in the arguments to dismiss uric acid as a risk factor for CKD. The greatest assumption was that the mechanism by which uric acid would cause kidney disease would be via the precipitation as crystals in the kidney, similar to the way it causes gout. However, when laboratory animals with CKD were made hyperuricemic, the renal disease progressed rapidly despite an absence of crystals in the kidney. Since this seminal study, there has been a renewed interest in the potential role uric acid may have in both acute and CKD. We briefly review some of the major advances that have occurred in this field in the last 15 years.
Keywords: allopurinol; chronic kidney disease; gout; hyperuricemia; uric acid.
Figures
References
-
- Johnson G. On the Diseases of the Kidney. London: John W Parker and Son; 1852.
-
- Talbott JH, Terplan KL. The kidney in gout. Medicine (Baltimore) 1960;39:405–467. - PubMed
-
- Barlow KA, Beilin LJ. Renal disease in primary gout. Q J Med. 1968;37:79–96. - PubMed
-
- Yu TF, Berger L. Impaired renal function gout: its association with hypertensive vascular disease and intrinsic renal disease. Am J Med. 1982;72:95–100. - PubMed
-
- Johnson RJ, Kivlighn SD, Kim YG, et al. Reappraisal of the pathogenesis and consequences of hyperuricemia in hypertension, cardiovascular disease, and renal disease. Am J Kidney Dis. 1999;33:225–234. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
