

Estrogen plus progestin and breast cancer incidence and mortality in the Women's Health Initiative Observational Study
- PMID: 23543779
- PMCID: PMC3691942
- DOI: 10.1093/jnci/djt043
Estrogen plus progestin and breast cancer incidence and mortality in the Women's Health Initiative Observational Study
Abstract
Background: In the Women's Health Initiative (WHI) randomized trial, estrogen plus progestin increased both breast cancer incidence and mortality. In contrast, most observational studies associate estrogen plus progestin with favorable prognosis breast cancers. To address differences, a cohort of WHI observational study participants with characteristics similar to the WHI clinical trial was studied.
Methods: We identified 41 449 postmenopausal women with no prior hysterectomy and mammogram negative within 2 years who were either not hormone users (n = 25 328) or estrogen and progestin users (n = 16 121). Multivariable-adjusted Cox proportional hazard regression was used to calculate hazard ratios (HRs) with 95% confidence intervals (CI). All statistical tests were two-sided.
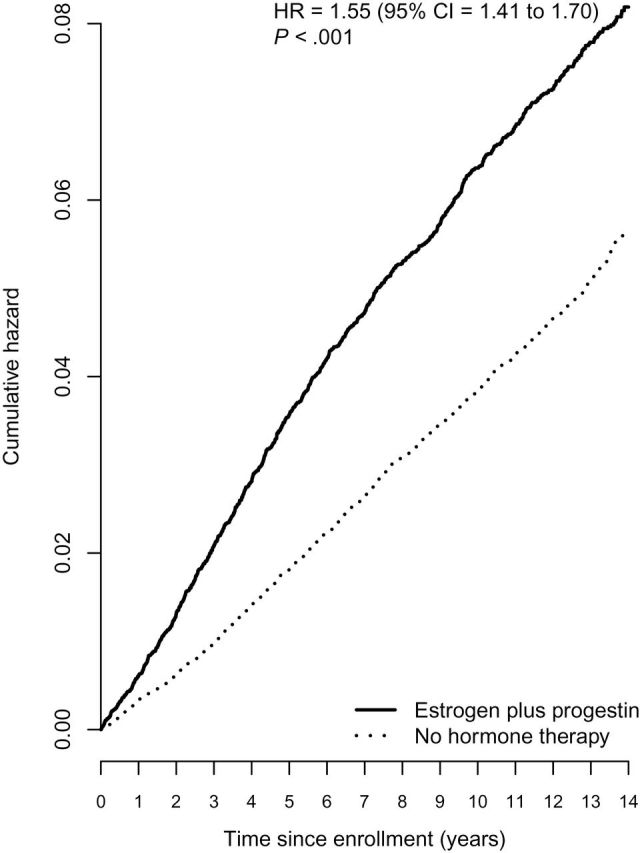
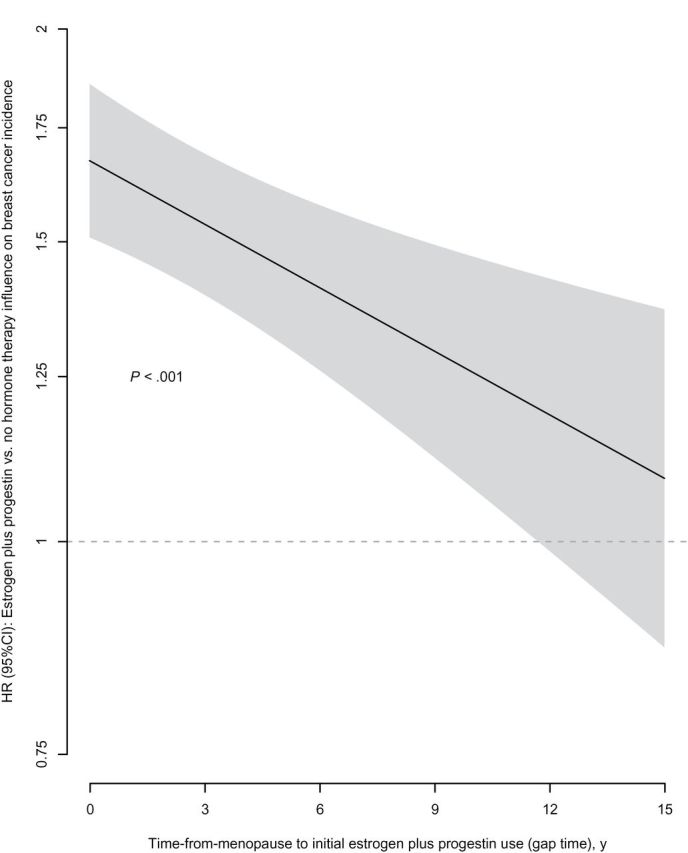
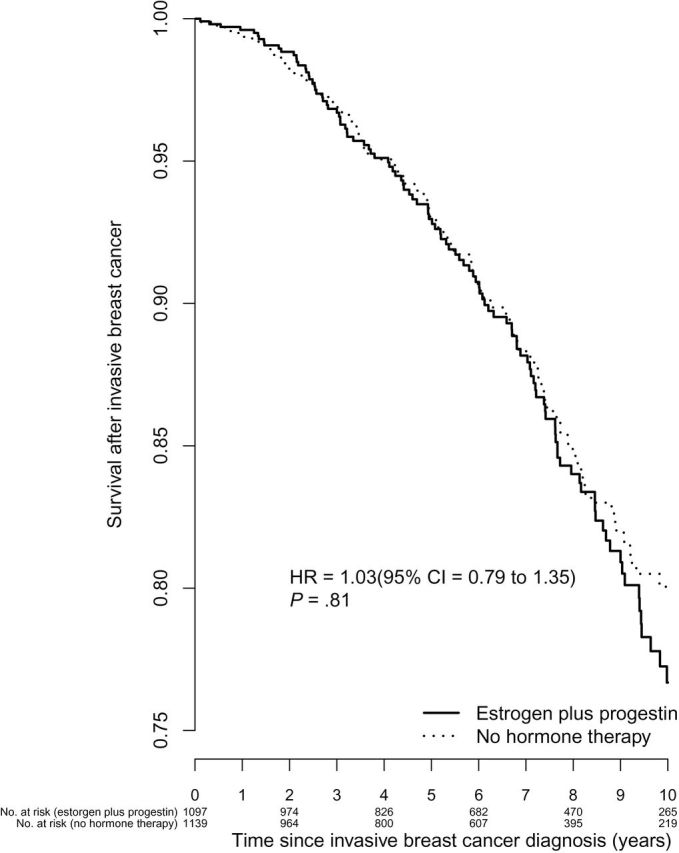
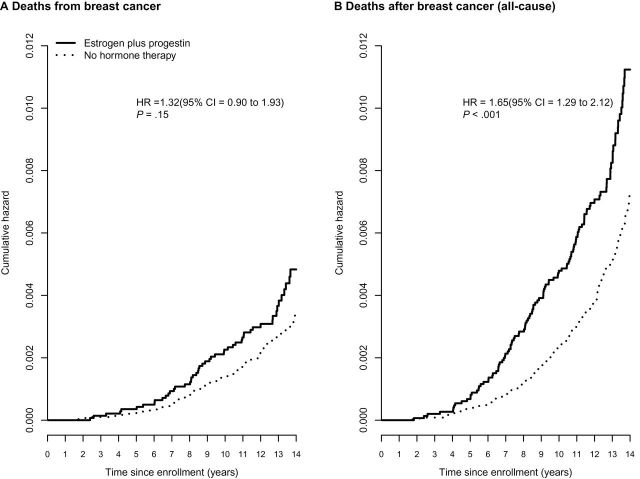
Results: After a mean of 11.3 (SD = 3.1) years, with 2236 breast cancers, incidence was higher in estrogen plus progestin users than in nonusers (0.60% vs 0.42%, annualized rate, respectively; HR = 1.55, 95% CI = 1.41 to 1.70, P < .001). Women initiating hormone therapy closer to menopause had higher breast cancer risk with linear diminishing influence as time from menopause increased (P < .001). Survival after breast cancer, measured from diagnosis, was similar in combined hormone therapy users and nonusers (HR = 1.03, 95% CI = 0.79 to 1.35). On a population basis, there were somewhat more deaths from breast cancer, measured from cohort entry (HR = 1.32, 95% CI = 0.90 to 1.93, P = .15), and more all-cause deaths after breast cancer (HR = 1.65, 95% CI = 1.29 to 2.12, P < .001) in estrogen plus progestin users than in nonusers.
Conclusions: Consistent with WHI randomized trial findings, estrogen plus progestin use is associated with increased breast cancer incidence. Because prognosis after diagnosis on combined hormone therapy is similar to that of nonusers, increased breast cancer mortality can be expected.
Figures
Comment in
-
The effect of estrogen plus progestin hormone therapy on breast cancer mortality: still unresolved.J Natl Cancer Inst. 2013 Apr 17;105(8):513-4. doi: 10.1093/jnci/djt058. Epub 2013 Mar 29. J Natl Cancer Inst. 2013. PMID: 23543780 No abstract available.
-
Re: Estrogen plus progestin and breast cancer incidence and mortality in the women's health initiative observational study.J Natl Cancer Inst. 2014 Feb;106(2):djt372. doi: 10.1093/jnci/djt372. Epub 2013 Dec 22. J Natl Cancer Inst. 2014. PMID: 24363446 No abstract available.
References
-
- Chlebowski RT, Hendrix SL, Langer RD, et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative randomized trial. JAMA. 2003; 289(24):3243–3253 - PubMed
-
- Colditz GA, Hankinson SE, Hunter DJ, et al. The use of estrogens and progestins and the risk of breast cancer in postmenopausal women. N Engl J Med. 1995; 332(24):1589–1593 - PubMed
-
- Bergkvist L, Adami HO, Persson J, et al. Prognosis after breast cancer diagnosis in women exposed to estrogen and estrogen-progestogen replacement therapy. Am J Epidemiol. 1989; 130(2):221–228 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
