

In Vitro and In Vivo Analysis of RTK Inhibitor Efficacy and Identification of Its Novel Targets in Glioblastomas
- PMID: 23544171
- PMCID: PMC3610556
- DOI: 10.1593/tlo.12400
In Vitro and In Vivo Analysis of RTK Inhibitor Efficacy and Identification of Its Novel Targets in Glioblastomas
Abstract
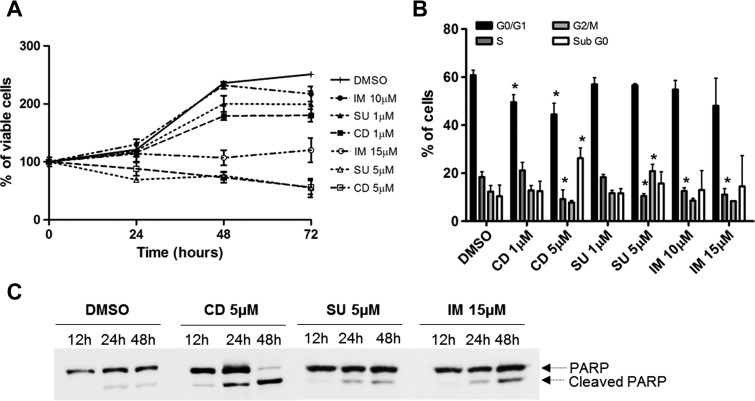
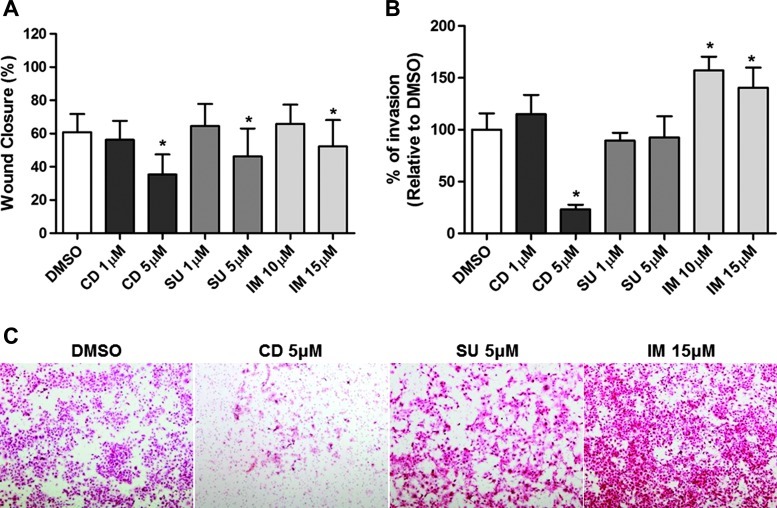
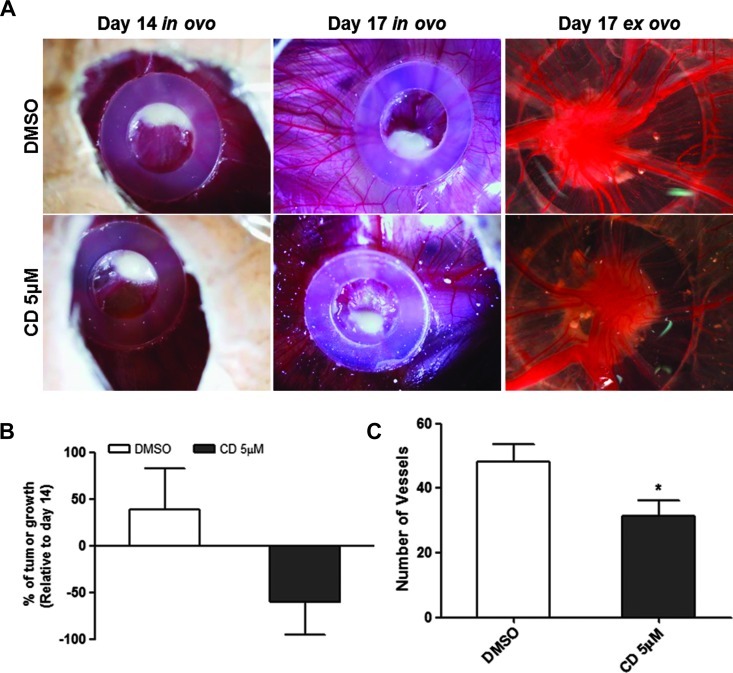
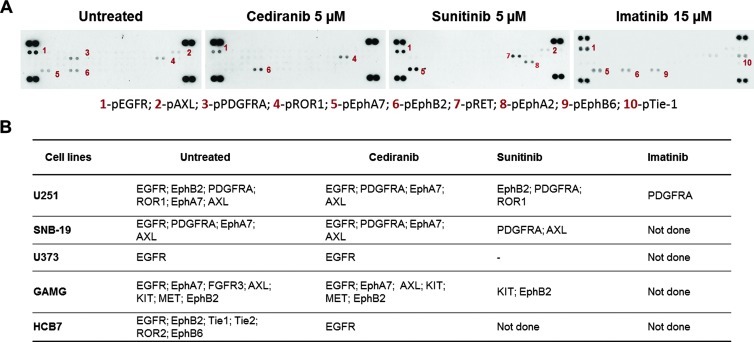
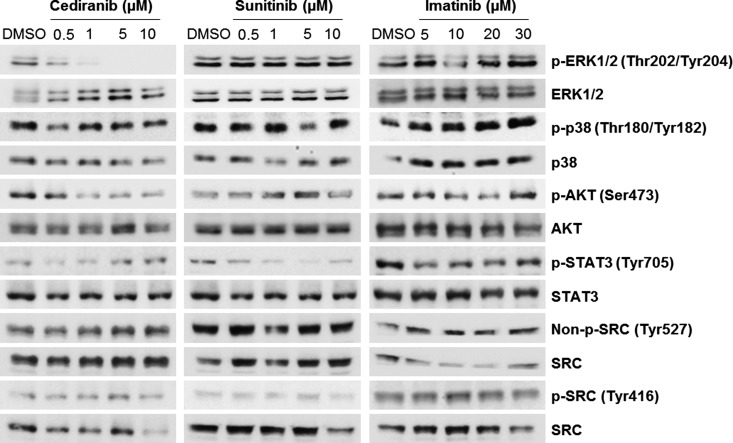
Treatment for glioblastoma consists of radiotherapy and temozolomide-based chemotherapy. However, virtually all patients recur, leading to a fatal outcome. Receptor tyrosine kinase (RTK)-targeted therapy has been the focus of attention in novel treatment options for these patients. Here, we compared the efficacy of imatinib, sunitinib, and cediranib in glioblastoma models. In the present work, the biologic effect of the drugs was screened by viability, cell cycle, apoptosis, migration, and invasion in vitro assays or in vivo by chick chorioallantoic membrane assay. Intracellular signaling was assessed by Western blot and the RTK targets were identified using phospho-RTK arrays. The amplified status of KIT, PDGFRA, and VEGFR2 genes was assessed by quantitative polymerase chain reaction. In a panel of 10 glioblastoma cell lines, we showed that cediranib was the most potent. In addition, cediranib and sunitinib synergistically sensitize the cells to temozolomide. Cediranib efficacy was shown to associate with higher cytostatic and unique cytotoxic effects in vitro and both antitumoral and antiangiogenic activity in vivo, which could associate with its great capacity to inhibit mitogen-activated protein kinase (MAPK) and AKT pathways. The molecular status of KIT, PDGFRA, and VEGFR2 did not predict glioblastoma cell responsiveness to any of the RTK inhibitors. Importantly, phospho-RTK arrays revealed novel targets for cediranib and sunitinib therapy. In conclusion, the novel targets found may be of value as future biomarkers for therapy response in glioblastoma and lead to the rational selection of patients for effective molecular targeted treatment.
Figures
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. - PubMed
-
- Wen PY, Kesari S. Malignant gliomas in adults. N Engl J Med. 2008;359:492–507. - PubMed
-
- Huse JT, Holland EC. Targeting brain cancer: advances in the molecular pathology of malignant glioma and medulloblastoma. Nat Rev Cancer. 2010;10:319–331. - PubMed
-
- Niyazi M, Siefert A, Schwarz SB, Ganswindt U, Kreth FW, Tonn JC, Belka C. Therapeutic options for recurrent malignant glioma. Radiother Oncol. 2011;98:1–14. - PubMed
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. - PubMed
Supplementary References
-
- Martinho O, Longatto-Filho A, Lambros MB, Martins A, Pinheiro C, Silva A, Pardal F, Amorim J, Mackay A, Milanezi F, et al. Expression, mutation and copy number analysis of platelet-derived growth factor receptor A (PDGFRA) and its ligand PDGFA in gliomas. Br J Cancer. 2009;101:973–982. - PMC - PubMed
-
- Martinho O, Goncalves A, Moreira MA, Ribeiro LF, Queiroz GS, Schmitt FC, Reis RM, Longatto-Filho A. KIT activation in uterine cervix adenosquamous carcinomas by KIT/SCF autocrine/paracrine stimulation loops. Gynecol Oncol. 2008;111:350–355. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous