

doi: 10.1007/s10689-013-9637-8.
The history of Lynch syndrome
Affiliations
- PMID: 23546821
- PMCID: PMC3720817
- DOI: 10.1007/s10689-013-9637-8
Item in Clipboard
The history of Lynch syndrome
Fam Cancer.
2013 Jun.
No abstract available
Conflict of interest statement
The authors have no conflicts of interest to report
Figures

Photos of A. S. Warthin, M.D., Ph.D. A. Photo of Warthin as a young man, about 1900 B. Formal photo of Warthin, date uncertain. C. Informal photo of Warthin, date uncertain . D. Warthin at his desk, date uncertain.

Photos of A. S. Warthin, M.D., Ph.D. A. Photo of Warthin as a young man, about 1900 B. Formal photo of Warthin, date uncertain. C. Informal photo of Warthin, date uncertain . D. Warthin at his desk, date uncertain.

Photos of A. S. Warthin, M.D., Ph.D. A. Photo of Warthin as a young man, about 1900 B. Formal photo of Warthin, date uncertain. C. Informal photo of Warthin, date uncertain . D. Warthin at his desk, date uncertain.

Photos of A. S. Warthin, M.D., Ph.D. A. Photo of Warthin as a young man, about 1900 B. Formal photo of Warthin, date uncertain. C. Informal photo of Warthin, date uncertain . D. Warthin at his desk, date uncertain.

A. Warthin’s initial pedigree of Cancer Family G, from his seminal article in the Arch Int Med, 1913
. Note the predominance of uterine and gastric cancers in the earlier generations. B. Photo of the immigrant founder of Family G. He had 10 children, 6 of whom developed cancer. He died in 1856 at age 60, of cancer. By the third generation, there were 70 descendents, 33 of whom had developed uterine, gastric or colon cancer.

A. Warthin’s initial pedigree of Cancer Family G, from his seminal article in the Arch Int Med, 1913
. Note the predominance of uterine and gastric cancers in the earlier generations. B. Photo of the immigrant founder of Family G. He had 10 children, 6 of whom developed cancer. He died in 1856 at age 60, of cancer. By the third generation, there were 70 descendents, 33 of whom had developed uterine, gastric or colon cancer.

Henry T. Lynch, M.D.

A. “Cancer Family G Revisited”, pedigree from the 1971 article by Lynch that updated the index family with follow-up on 650 family members. B. As Lynch added information, the data on subsequent cancers increased with each successive generation, as noted. C. Lynch continued with the pedigree, annotating additional tumors over time, resulting in this circular pedigree.

A. “Cancer Family G Revisited”, pedigree from the 1971 article by Lynch that updated the index family with follow-up on 650 family members. B. As Lynch added information, the data on subsequent cancers increased with each successive generation, as noted. C. Lynch continued with the pedigree, annotating additional tumors over time, resulting in this circular pedigree.
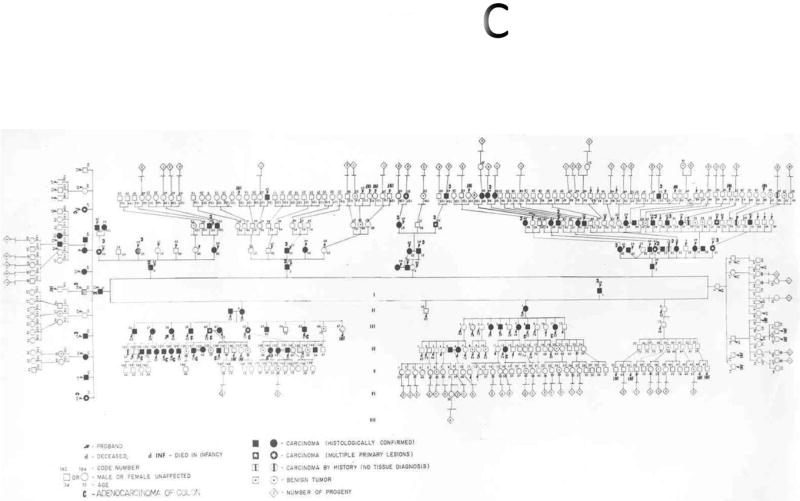
A. “Cancer Family G Revisited”, pedigree from the 1971 article by Lynch that updated the index family with follow-up on 650 family members. B. As Lynch added information, the data on subsequent cancers increased with each successive generation, as noted. C. Lynch continued with the pedigree, annotating additional tumors over time, resulting in this circular pedigree.

Discovery of MSI A. The laboratory of Manuel Perucho, PhD was hunting for allelic losses and gains in colorectal cancer tissues using arbitrarily primed PCR, published in 1992 . This was a powerful technique for finding copy number changes and LOH as they ran the autoradiograms from cancer tissues and normal colon samples side-by-side looking for bands present in normal tissue that were fainter or stronger in the cancer. In 1993, they detected small deletions in the PCR products, as indicated by the arrowheads, using several different arbitrary primers and primer pairs (listed as primers A, A+B, B, B+C, and C, along the top) on DNA from normal colons (N) and matched samples of tumor (T) . B. The novel bands were cut from the original gels and sequenced. The altered bands contained mononucleotide repeats (a poly-T microsatellite sequence, indicated by the brackets), and the DNA from the tumor (T) harbored deletions in the repeat tract.
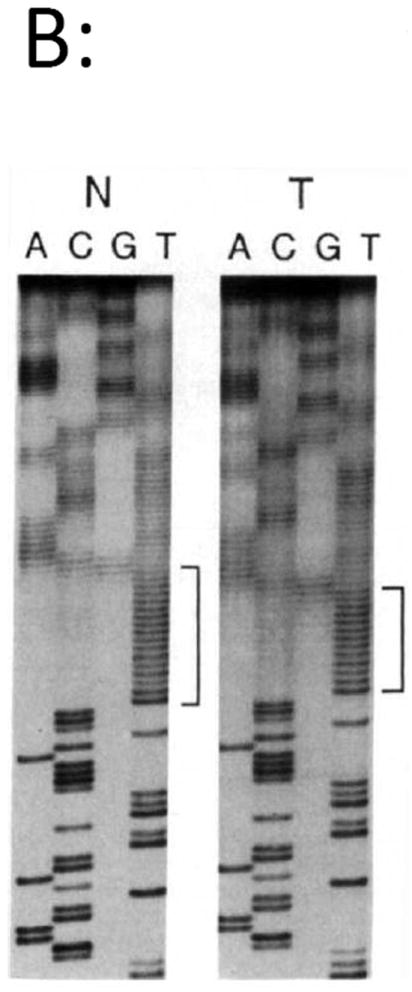
Discovery of MSI A. The laboratory of Manuel Perucho, PhD was hunting for allelic losses and gains in colorectal cancer tissues using arbitrarily primed PCR, published in 1992 . This was a powerful technique for finding copy number changes and LOH as they ran the autoradiograms from cancer tissues and normal colon samples side-by-side looking for bands present in normal tissue that were fainter or stronger in the cancer. In 1993, they detected small deletions in the PCR products, as indicated by the arrowheads, using several different arbitrary primers and primer pairs (listed as primers A, A+B, B, B+C, and C, along the top) on DNA from normal colons (N) and matched samples of tumor (T) . B. The novel bands were cut from the original gels and sequenced. The altered bands contained mononucleotide repeats (a poly-T microsatellite sequence, indicated by the brackets), and the DNA from the tumor (T) harbored deletions in the repeat tract.

Lynch Syndrome kindreds are linked to chromosome 2p and MSI A. In 1993, the international consortium organized by Vogelstein, de la Chapelle and others had identified familial CRC kindreds as shown in the pedigrees. Two had significant linkage between CRC and the microsatellite marker D2S123, located on chromosome 2p . B. The investigators used the microsatellite marker D2S123, looking for LOH in the CRC tissue DNA. Instead of LOH, they found MSI as shown by the anomalously migrating bands indicated by the arrowheads .

Lynch Syndrome kindreds are linked to chromosome 2p and MSI A. In 1993, the international consortium organized by Vogelstein, de la Chapelle and others had identified familial CRC kindreds as shown in the pedigrees. Two had significant linkage between CRC and the microsatellite marker D2S123, located on chromosome 2p . B. The investigators used the microsatellite marker D2S123, looking for LOH in the CRC tissue DNA. Instead of LOH, they found MSI as shown by the anomalously migrating bands indicated by the arrowheads .

Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.

Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.

Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.

Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.
Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.

Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.

Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.

Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.

Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.

Key contributors to the field, in the modern era of molecular biology and genetics A. Hans Vasen, MD (Leiden University, The Netherlands). B. Manuel Perucho, PhD (Sanford-Burnham Medical Research Unit, La Jolla, CA). Discovered MSI, and proposed a novel pathway for CRC development. C. Stephen Thibodeau, PhD (Mayo Clinic, Minnesota). Independently discovered MSI, and suggested that these tumors evolved through a unique mechanism that did not involve LOH events. D. Bert Vogelstein, MD (Johns Hopkins University). Linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. E. Albert de la Chapelle, MD, PhD (The Ohio State University). Together with Vogelstein and others, linked MSI to hereditary colorectal cancer; identified several of the DNA MMR genes, and linked mutant MMR genes to Lynch Syndrome. F. Lauri Aaltonen, MD, PhD (University of Helsinki, Finland). Together with Vogelstein and de la Chapelle, made the critical observation that hereditary CRC was linked to a locus on chromosome 2p, and that there was MSI in the linkage marker, which was a microsatellite sequence. G. Richard Kolodner, PhD (University of California, San Diego). Cloned the human homologs of MSH2 and MLH1, and found germline mutations in families with Lynch Syndrome. H. Minoru Koi, PhD (Baylor University Medical Center, Dallas, TX). Created the first in vitro models of Lynch Syndrome from the HCT116 cell line, using stable chromosome transfer to correct the DNA MMR defect. I. C. Richard Boland, MD (Baylor University Medical Center, Dallas, TX). Studied hereditary colon cancer as a medical student, coined the term “Lynch Syndrome”, used the cell model developed by Koi in a series of studies on the response of DNA MMR deficient cells to chemotherapeutic drugs. J. Sir John Burn, MD, reported the first effective medical intervention for Lynch Syndrome – aspirin.
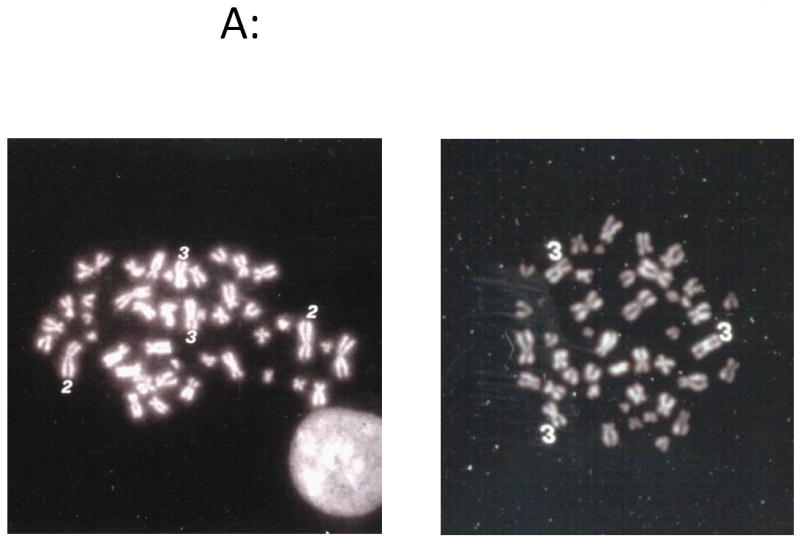
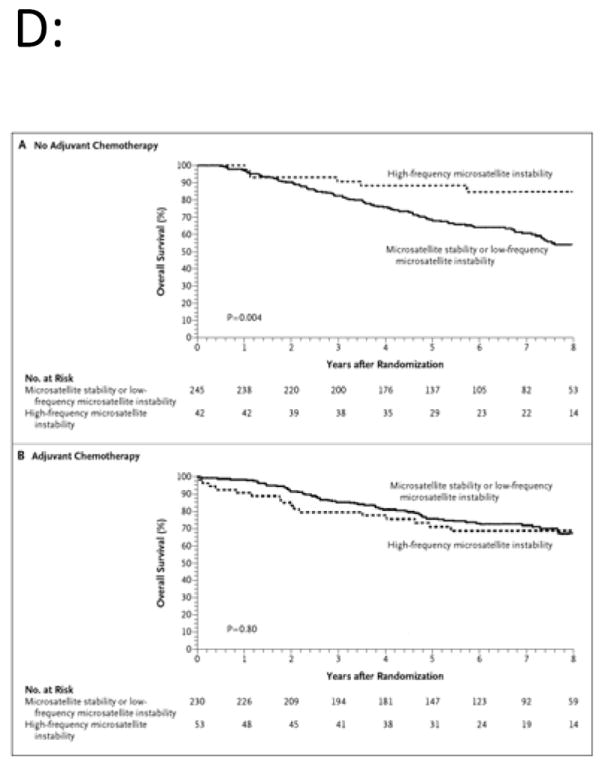
DNA MMR deficiency and response to chemotherapeutic agents. A. In early 1994, Minoru Koi, PhD created a DNA MMR-corrected model by stably transferring a copy of human chromosome 3 into the MLH1-deficient CRC cell line HCT116, which is diploid. On the left is a karyotype of the uncorrected cell line, with 2 copies of both chromosomes 2 and 3; this cell line is DNA MMR deficient and has MSI. On the right is HCT116+chr3, which has 3 copies of chromosome 3, the MSI has been corrected, and the cell line is MMR proficient , . B. The CRC cell lines that are MMR deficient (as shown in the circle) can tolerate increasing doses of the alkylating agent MNNG, which damages DNA, as shown in the cells that continue to have high cloning efficiency (HCT116, HCT116+chr2, LoVo, 2774, and HCT116+chr3M2). However, the cell lines that are DNA MMR proficient (shown in the square) are sensitive to DNA damage, and cannot be grown in 5 M MNNG (the lower 2 lines are HCT116+chr3 and SW480) . C. The MMR-deficient cell line SW48 has undergone methylation-induced silencing of MLH1, which is reversed by the demethylating drug 5azadC. The upper curves (in the circle) show that DNA MMR-deficient cells (SW84, HCT116, HTC116+chr2) can tolerate up to 5 M 5-FU, but MMR-proficient cells, such as HCT116+chr3 or SW48 after demethylation) cannot (shown in the rectangle). This in vitro experiment suggested that MMR-deficient tumors may not have the same response to chemotherapy as MMR-proficient ones, . D. In 2003, a retrospective study of CRC patients prospectively randomized to receive either 5-FU-based adjuvant chemotherapy or not, analyzed outcomes according to MSI status. The upper panel shows that patients with MSI CRCs had a better outcome than those without MSI if they did not receive chemotherapy. However, those randomized to receive 5-FU-based chemotherapy lost the survival benefit based upon MSI, and the two survival curves collapsed, with slight increase in mortality among the treated patients.

DNA MMR deficiency and response to chemotherapeutic agents. A. In early 1994, Minoru Koi, PhD created a DNA MMR-corrected model by stably transferring a copy of human chromosome 3 into the MLH1-deficient CRC cell line HCT116, which is diploid. On the left is a karyotype of the uncorrected cell line, with 2 copies of both chromosomes 2 and 3; this cell line is DNA MMR deficient and has MSI. On the right is HCT116+chr3, which has 3 copies of chromosome 3, the MSI has been corrected, and the cell line is MMR proficient , . B. The CRC cell lines that are MMR deficient (as shown in the circle) can tolerate increasing doses of the alkylating agent MNNG, which damages DNA, as shown in the cells that continue to have high cloning efficiency (HCT116, HCT116+chr2, LoVo, 2774, and HCT116+chr3M2). However, the cell lines that are DNA MMR proficient (shown in the square) are sensitive to DNA damage, and cannot be grown in 5 M MNNG (the lower 2 lines are HCT116+chr3 and SW480) . C. The MMR-deficient cell line SW48 has undergone methylation-induced silencing of MLH1, which is reversed by the demethylating drug 5azadC. The upper curves (in the circle) show that DNA MMR-deficient cells (SW84, HCT116, HTC116+chr2) can tolerate up to 5 M 5-FU, but MMR-proficient cells, such as HCT116+chr3 or SW48 after demethylation) cannot (shown in the rectangle). This in vitro experiment suggested that MMR-deficient tumors may not have the same response to chemotherapy as MMR-proficient ones, . D. In 2003, a retrospective study of CRC patients prospectively randomized to receive either 5-FU-based adjuvant chemotherapy or not, analyzed outcomes according to MSI status. The upper panel shows that patients with MSI CRCs had a better outcome than those without MSI if they did not receive chemotherapy. However, those randomized to receive 5-FU-based chemotherapy lost the survival benefit based upon MSI, and the two survival curves collapsed, with slight increase in mortality among the treated patients.

DNA MMR deficiency and response to chemotherapeutic agents. A. In early 1994, Minoru Koi, PhD created a DNA MMR-corrected model by stably transferring a copy of human chromosome 3 into the MLH1-deficient CRC cell line HCT116, which is diploid. On the left is a karyotype of the uncorrected cell line, with 2 copies of both chromosomes 2 and 3; this cell line is DNA MMR deficient and has MSI. On the right is HCT116+chr3, which has 3 copies of chromosome 3, the MSI has been corrected, and the cell line is MMR proficient , . B. The CRC cell lines that are MMR deficient (as shown in the circle) can tolerate increasing doses of the alkylating agent MNNG, which damages DNA, as shown in the cells that continue to have high cloning efficiency (HCT116, HCT116+chr2, LoVo, 2774, and HCT116+chr3M2). However, the cell lines that are DNA MMR proficient (shown in the square) are sensitive to DNA damage, and cannot be grown in 5 M MNNG (the lower 2 lines are HCT116+chr3 and SW480) . C. The MMR-deficient cell line SW48 has undergone methylation-induced silencing of MLH1, which is reversed by the demethylating drug 5azadC. The upper curves (in the circle) show that DNA MMR-deficient cells (SW84, HCT116, HTC116+chr2) can tolerate up to 5 M 5-FU, but MMR-proficient cells, such as HCT116+chr3 or SW48 after demethylation) cannot (shown in the rectangle). This in vitro experiment suggested that MMR-deficient tumors may not have the same response to chemotherapy as MMR-proficient ones, . D. In 2003, a retrospective study of CRC patients prospectively randomized to receive either 5-FU-based adjuvant chemotherapy or not, analyzed outcomes according to MSI status. The upper panel shows that patients with MSI CRCs had a better outcome than those without MSI if they did not receive chemotherapy. However, those randomized to receive 5-FU-based chemotherapy lost the survival benefit based upon MSI, and the two survival curves collapsed, with slight increase in mortality among the treated patients.
DNA MMR deficiency and response to chemotherapeutic agents. A. In early 1994, Minoru Koi, PhD created a DNA MMR-corrected model by stably transferring a copy of human chromosome 3 into the MLH1-deficient CRC cell line HCT116, which is diploid. On the left is a karyotype of the uncorrected cell line, with 2 copies of both chromosomes 2 and 3; this cell line is DNA MMR deficient and has MSI. On the right is HCT116+chr3, which has 3 copies of chromosome 3, the MSI has been corrected, and the cell line is MMR proficient , . B. The CRC cell lines that are MMR deficient (as shown in the circle) can tolerate increasing doses of the alkylating agent MNNG, which damages DNA, as shown in the cells that continue to have high cloning efficiency (HCT116, HCT116+chr2, LoVo, 2774, and HCT116+chr3M2). However, the cell lines that are DNA MMR proficient (shown in the square) are sensitive to DNA damage, and cannot be grown in 5 M MNNG (the lower 2 lines are HCT116+chr3 and SW480) . C. The MMR-deficient cell line SW48 has undergone methylation-induced silencing of MLH1, which is reversed by the demethylating drug 5azadC. The upper curves (in the circle) show that DNA MMR-deficient cells (SW84, HCT116, HTC116+chr2) can tolerate up to 5 M 5-FU, but MMR-proficient cells, such as HCT116+chr3 or SW48 after demethylation) cannot (shown in the rectangle). This in vitro experiment suggested that MMR-deficient tumors may not have the same response to chemotherapy as MMR-proficient ones, . D. In 2003, a retrospective study of CRC patients prospectively randomized to receive either 5-FU-based adjuvant chemotherapy or not, analyzed outcomes according to MSI status. The upper panel shows that patients with MSI CRCs had a better outcome than those without MSI if they did not receive chemotherapy. However, those randomized to receive 5-FU-based chemotherapy lost the survival benefit based upon MSI, and the two survival curves collapsed, with slight increase in mortality among the treated patients.
References
-
- Warthin AS. Heredity with reference to carcinoma as shown by the study of the cases examined in the Pathological Laboratory of the University of Michigan, 1895-1912. Arch Int Med. 1913;12:546–555.
-
- Warthin AS. The further study of a cancer family. J Cancer Research. 1925;9:279–286.
-
- Hauser IJ, Weller CV. A further report on the cancer family of Warthin. American Journal of Cancer. 1936;27:434–449.
-
- Bargen JA, Mayo CW, Giffin LA. Familial trends in human cancer. J Heredity. 1941;32:7.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
