

urinary biomarkers in relapsing antineutrophil cytoplasmic antibody-associated vasculitis
- PMID: 23547217
- PMCID: PMC4505819
- DOI: 10.3899/jrheum.120879
urinary biomarkers in relapsing antineutrophil cytoplasmic antibody-associated vasculitis
Abstract
Objective: Glomerulonephritis (GN) is common in antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV), but tools for early detection of renal involvement are imperfect. We investigated 4 urinary proteins as markers of active renal AAV: alpha-1 acid glycoprotein (AGP), kidney injury molecule-1 (KIM-1), monocyte chemoattractant protein-1 (MCP-1), and neutrophil gelatinase-associated lipocalin (NGAL).
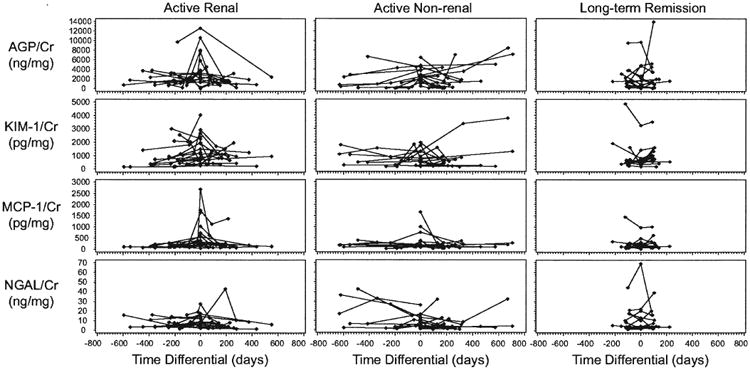
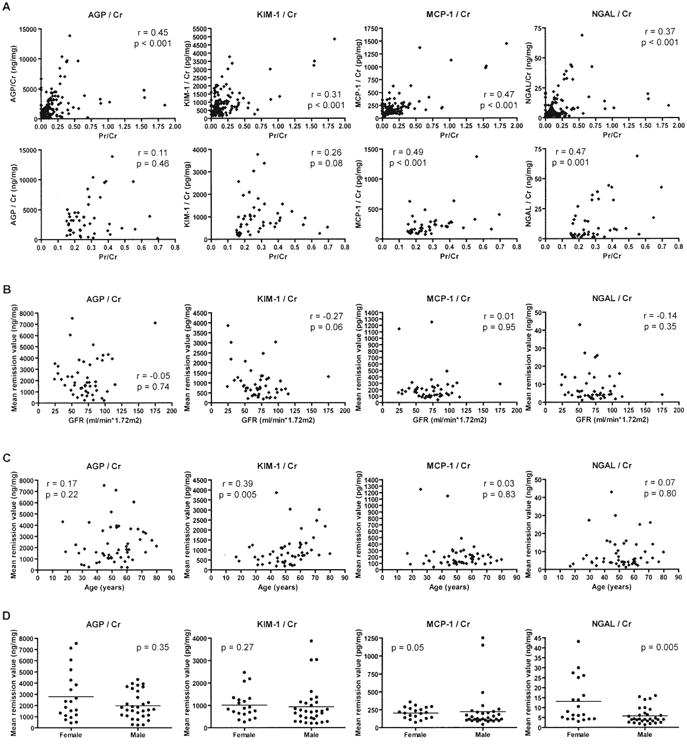
Methods: Patients with active renal AAV (n = 20), active nonrenal AAV (n = 16), and AAV in longterm remission (n = 14) were identified within a longitudinal cohort. Urinary biomarker concentrations (by ELISA) were normalized for urine creatinine. Marker levels during active AAV were compared to baseline remission levels (from 1-4 visits) for each patient. Areas under receiver-operating characteristic curves (AUC), sensitivities, specificities, and likelihood ratios (LR) comparing disease states were calculated.
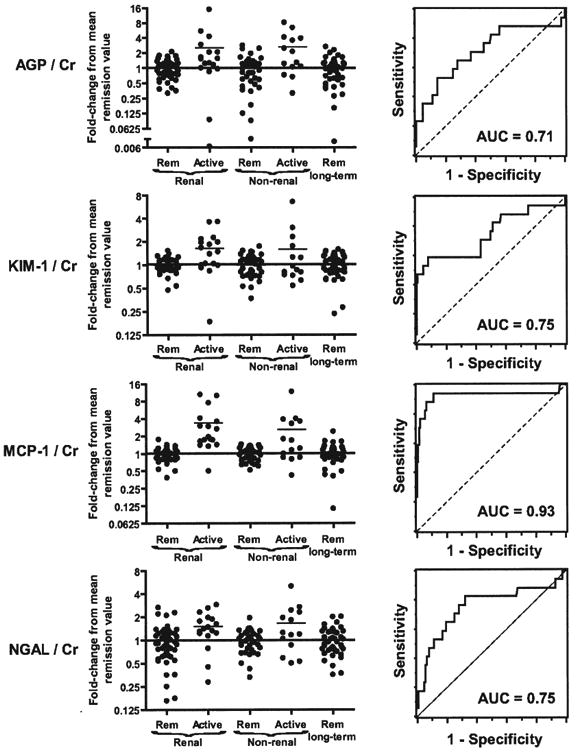
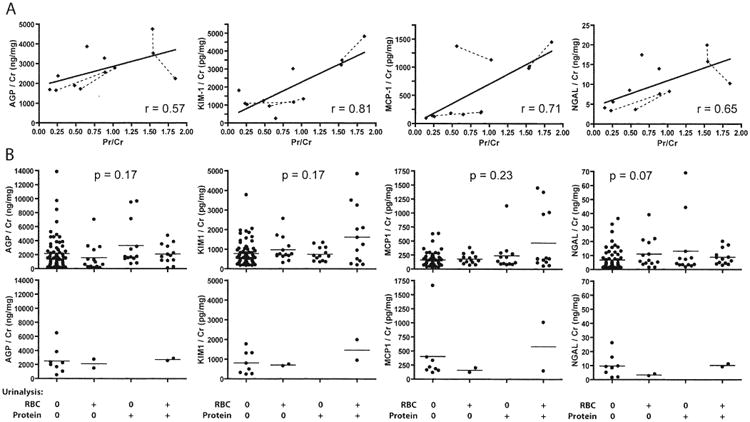
Results: Baseline biomarker levels varied among patients. All 4 markers increased during renal flares (p < 0.05). MCP-1 discriminated best between active renal disease and remission: a 1.3-fold increase in MCP-1 had 94% sensitivity and 89% specificity for active renal disease (AUC = 0.93, positive LR 8.5, negative LR 0.07). Increased MCP-1 also characterized 50% of apparently nonrenal flares. Change in AGP, KIM-1, or NGAL showed more modest ability to distinguish active renal disease from remission (AUC 0.71-0.75). Hematuria was noted in 83% of active renal episodes, but also 43% of nonrenal flares and 25% of remission samples.
Conclusion: Either urinary MCP-1 is not specific for GN in AAV, or it identifies early GN not detected by standard assessment and thus has potential to improve care. A followup study with kidney biopsy as the gold standard is needed.
Keywords: BIOMARKERS; GLOMERULONEPHRITIS; MONOCYTE CHEMOATTRACTANT PROTEIN-1; VASCULITIS; WEGENER GRANULOMATOSIS.
Figures
References
-
- Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med. 1992;116:488–98. - PubMed
-
- Reinhold-Keller E, Beuge N, Latza U, de Groot K, Rudert H, Nolle B, et al. An interdisciplinary approach to the care of patients with Wegener's granulomatosis: long-term outcome in 155 patients. Arthritis Rheum. 2000;43:1021–32. - PubMed
-
- Booth AD, Almond MK, Burns A, Ellis P, Gaskin G, Neild GH, et al. Outcome of ANCA-associated renal vasculitis: a 5-year retrospective study. Am J Kidney Dis. 2003;41:776–84. - PubMed
-
- Guillevin L, Cohen P, Gayraud M, Lhote F, Jarrousse B, Casassus P. Churg-Strauss syndrome. Clinical study and long-term follow-up of 96 patients. Medicine. 1999;78:26–37. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous