

A pilot study of the effect of spironolactone therapy on exercise capacity and endothelial dysfunction in pulmonary arterial hypertension: study protocol for a randomized controlled trial
- PMID: 23547564
- PMCID: PMC3653687
- DOI: 10.1186/1745-6215-14-91
A pilot study of the effect of spironolactone therapy on exercise capacity and endothelial dysfunction in pulmonary arterial hypertension: study protocol for a randomized controlled trial
Abstract
Background: Pulmonary arterial hypertension is a rare disorder associated with poor survival. Endothelial dysfunction plays a central role in the pathogenesis and progression of pulmonary arterial hypertension. Inflammation appears to drive this dysfunctional endothelial phenotype, propagating cycles of injury and repair in genetically susceptible patients with idiopathic and disease-associated pulmonary arterial hypertension. Therapy targeting pulmonary vascular inflammation to interrupt cycles of injury and repair and thereby delay or prevent right ventricular failure and death has not been tested. Spironolactone, a mineralocorticoid and androgen receptor antagonist, has been shown to improve endothelial function and reduce inflammation. Current management of patients with pulmonary arterial hypertension and symptoms of right heart failure includes use of mineralocorticoid receptor antagonists for their diuretic and natriuretic effects. We hypothesize that initiating spironolactone therapy at an earlier stage of disease in patients with pulmonary arterial hypertension could provide additional benefits through anti-inflammatory effects and improvements in pulmonary vascular function.
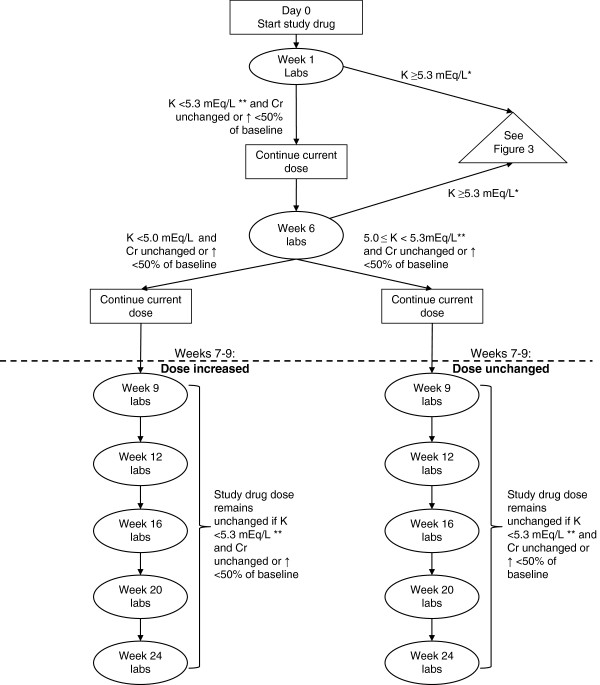
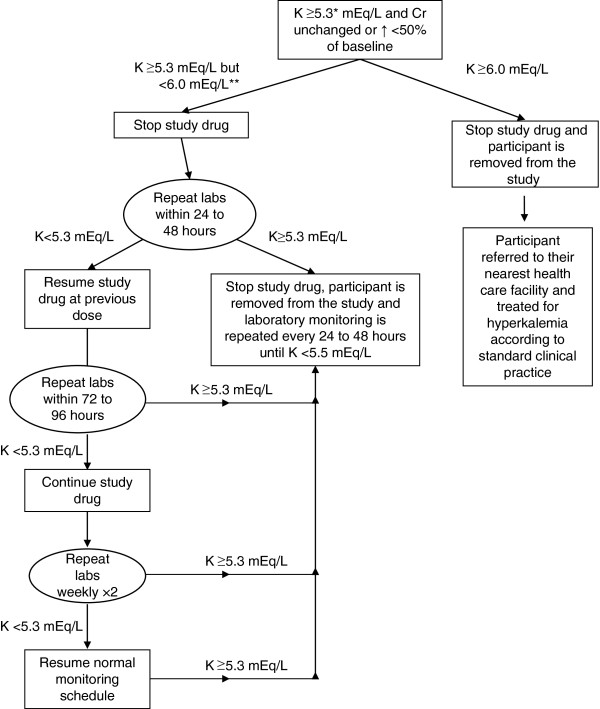
Methods/design: Seventy patients with pulmonary arterial hypertension without clinical evidence of right ventricular failure will be enrolled in a randomized, double-blinded, placebo-controlled trial to investigate the effect of early treatment with spironolactone on exercise capacity, clinical worsening and vascular inflammation in vivo. Our primary endpoint is change in placebo-corrected 6-minute walk distance at 24 weeks and the incidence of clinical worsening in the spironolactone group compared to placebo. At a two-sided alpha level of 0.05, we will have at least 84% power to detect an effect size (group mean difference divided by standard deviation) of 0.9 for the difference in the change of 6-minute walk distance from baseline between the two groups. Secondary endpoints include the effect of spironolactone on the change in placebo-corrected maximal oxygen consumption; plasma markers of vascular inflammation and peripheral blood mononuclear cell gene expression profiles; sympathetic nervous system activation, renin-angiotensin-aldosterone system activation and sex hormone metabolism; and right ventricular structure and function using echocardiography and novel high-resolution magnetic resonance imaging-based techniques. Safety and tolerability of spironolactone will be assessed with periodic monitoring for hyperkalemia and renal insufficiency as well as the incidence of drug discontinuation for untoward effects.
Trial registration: ClinicalTrials.gov: NCT01712620.
Figures
References
-
- Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, Elliott CG, Gaine SP, Gladwin MT, Jing ZC, Krowka MJ, Langleben D, Nakanishi N, Souza R. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54(1 Suppl):S43–54. - PubMed
-
- Badesch DB, Raskob GE, Elliott CG, Krichman AM, Farber HW, Frost AE, Barst RJ, Benza RL, Liou TG, Turner M, Giles S, Feldkircher K, Miller DP, McGoon MD. Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest. 2010;137(2):376–387. doi: 10.1378/chest.09-1140. - DOI - PubMed
-
- D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT, Levy PS, Pietra GG, Reid LM, Reeves JT, Rich S, Vreim CE, Williams GW, Wu M. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115(5):343–349. doi: 10.7326/0003-4819-115-5-343. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
