

Body mass index and incident coronary heart disease in women: a population-based prospective study
- PMID: 23547896
- PMCID: PMC3661394
- DOI: 10.1186/1741-7015-11-87
Body mass index and incident coronary heart disease in women: a population-based prospective study
Abstract
Background: A high body mass index (BMI) is associated with an increased risk of mortality from coronary heart disease (CHD); however, a low BMI may also be associated with an increased mortality risk. There is limited information on the relation of incident CHD risk across a wide range of BMI, particularly in women. We examined the relation between BMI and incident CHD overall and across different risk factors of the disease in the Million Women Study.
Methods: 1.2 million women (mean age=56 years) participants without heart disease, stroke, or cancer (except non-melanoma skin cancer) at baseline (1996 to 2001) were followed prospectively for 9 years on average. Adjusted relative risks and 20-year cumulative incidence from age 55 to 74 years were calculated for CHD using Cox regression.
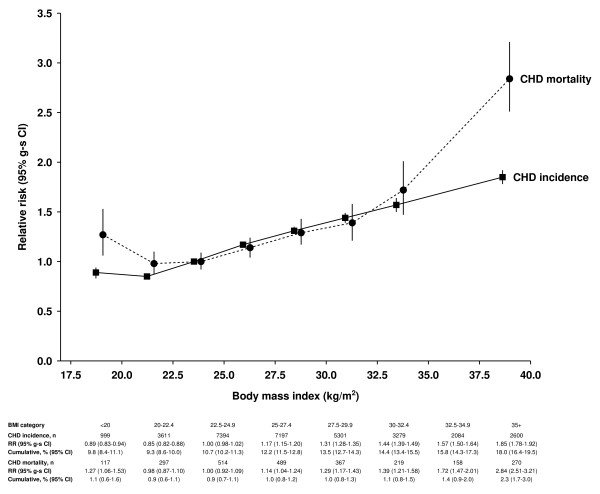
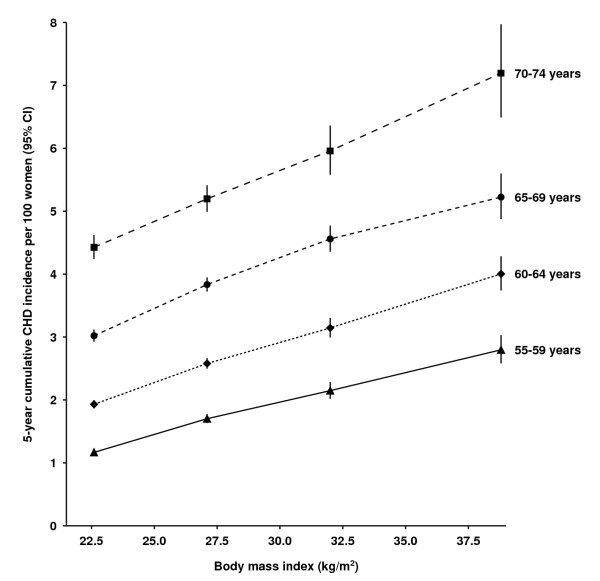
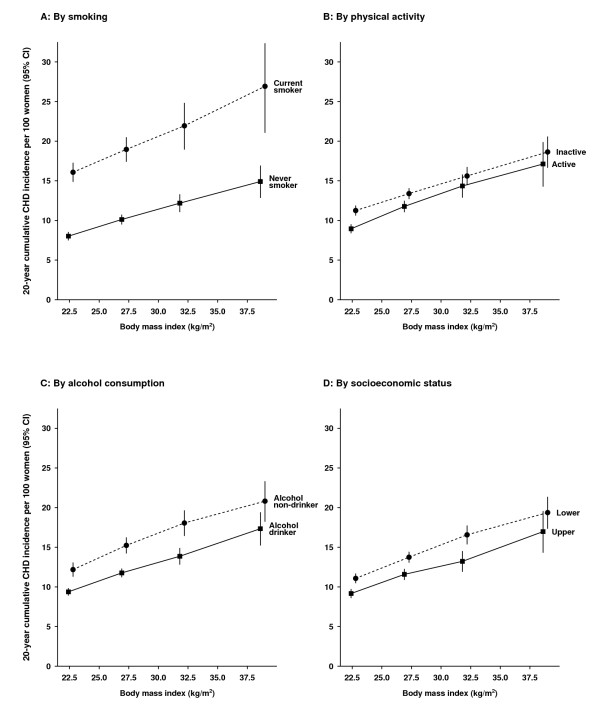
Results: After excluding the first 4 years of follow-up, we found that 32,465 women had a first coronary event (hospitalization or death) during follow-up. The adjusted relative risk for incident CHD per 5 kg/m2 increase in BMI was 1.23 (95% confidence interval (CI) 1.22 to 1.25). The cumulative incidence of CHD from age 55 to 74 years increased progressively with BMI, from 1 in 11 (95% CI 1 in 10 to 12) for BMI of 20 kg/m2, to 1 in 6(95% CI 1 in 5 to 7) for BMI of 34 kg/m2. A 10 kg/m2 increase in BMI conferred a similar risk to a 5-year increment in chronological age. The 20 year cumulative incidence increased with BMI in smokers and non-smokers, alcohol drinkers and non-drinkers, physically active and inactive, and in the upper and lower socioeconomic classes. In contrast to incident disease, the relation between BMI and CHD mortality (n=2,431) was J-shaped. For the less than 20 kg/m2 and ≥35 kg/m2 BMI categories, the respective relative risks were 1.27 (95% CI 1.06 to 1.53) and 2.84 (95% CI 2.51 to 3.21) for CHD deaths, and 0.89 (95% CI 0.83 to 0.94) and 1.85 (95% CI 1.78 to 1.92) for incident CHD.
Conclusions: CHD incidence in women increases progressively with BMI, an association consistently seen in different subgroups. The shape of the relation with BMI differs for incident and fatal disease.
Figures
References
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ. et al.Heart Disease and Stroke Statistics--2012 Update: a report From the American Heart Association. Circulation. 2012;125:e2–e220. - PMC - PubMed
-
- Scarborough P, Wickramasinghe K, Bhatnagar P, Smolina K, Mitchell C, Rayner M. Coronary Heart Disease Statistics, 2010 edition. London: British Heart Foundation; 2010.
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL. Global Burden of Disease and Risk Factors. New York: Oxford University Press; 2006. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
