

The malaria transition on the Arabian Peninsula: progress toward a malaria-free region between 1960-2010
- PMID: 23548086
- PMCID: PMC3951717
- DOI: 10.1016/B978-0-12-407706-5.00003-4
The malaria transition on the Arabian Peninsula: progress toward a malaria-free region between 1960-2010
Abstract
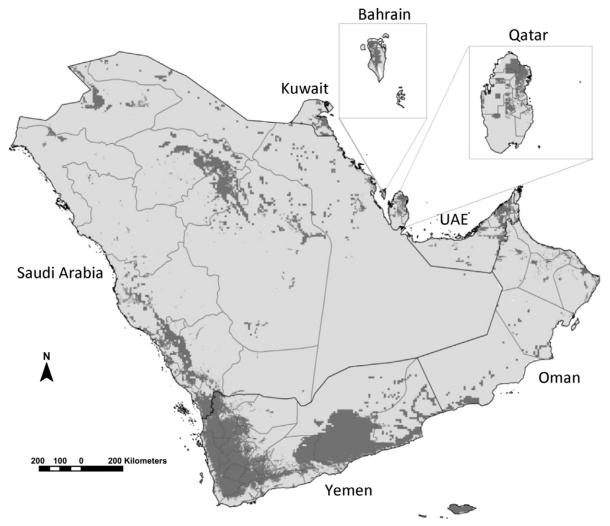
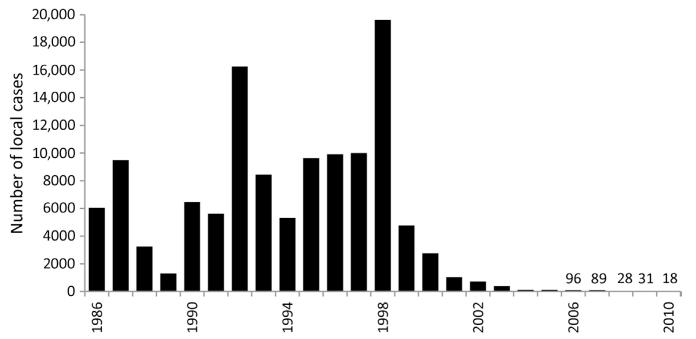
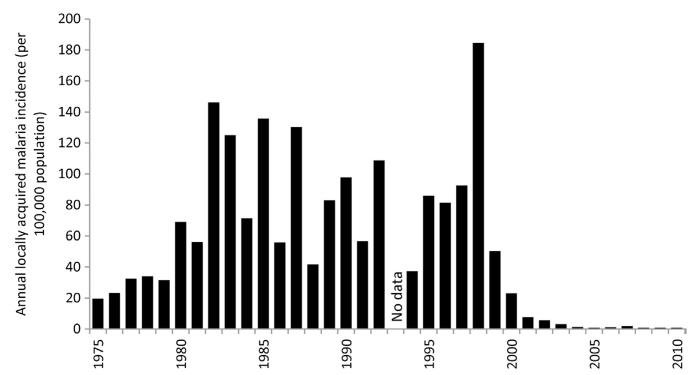
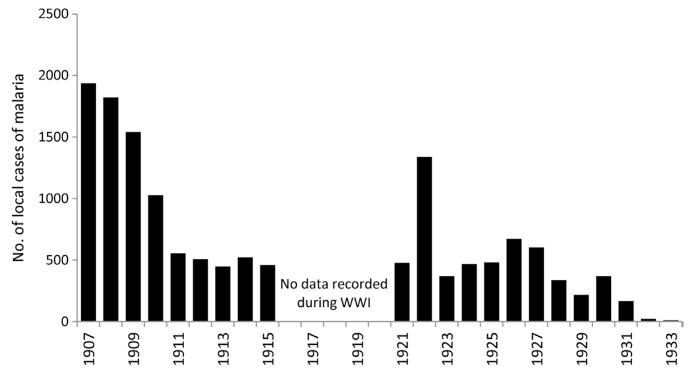
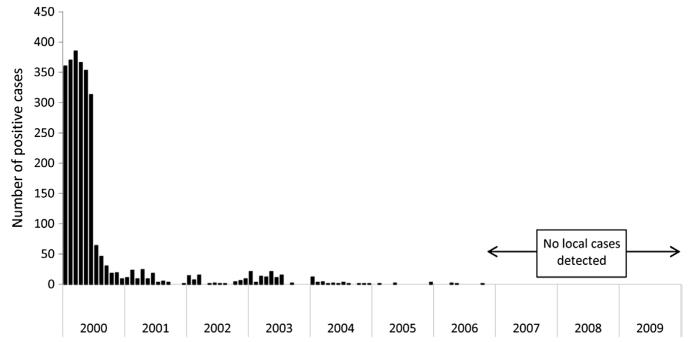
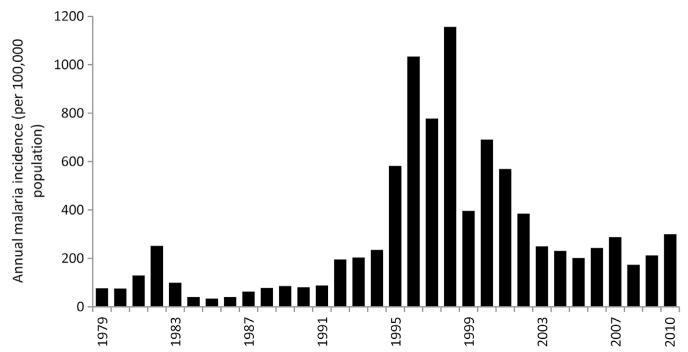
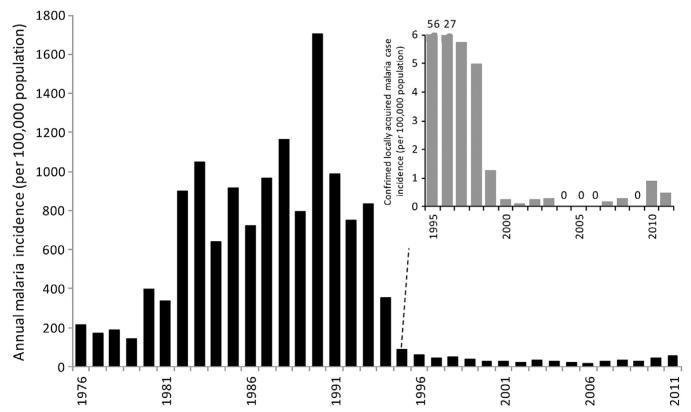
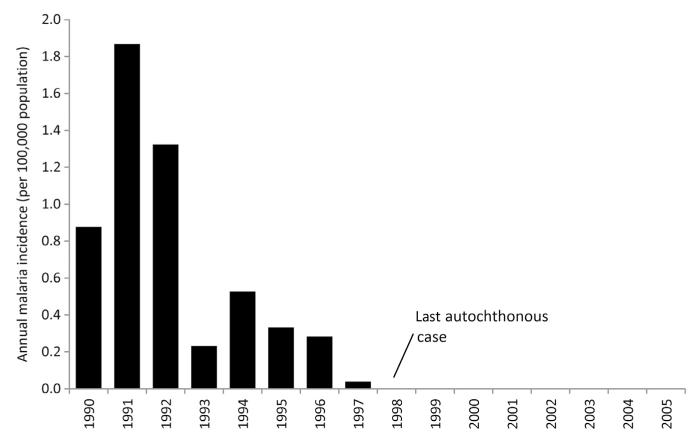
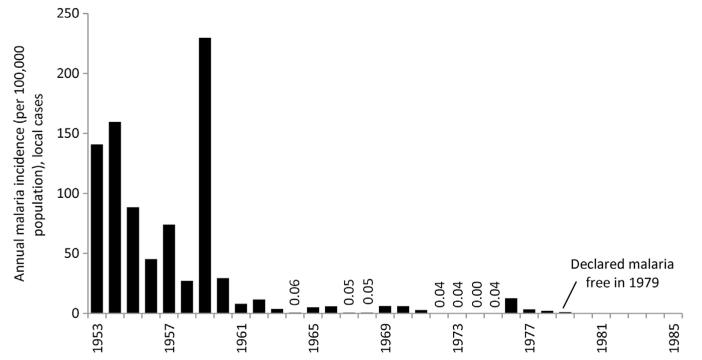
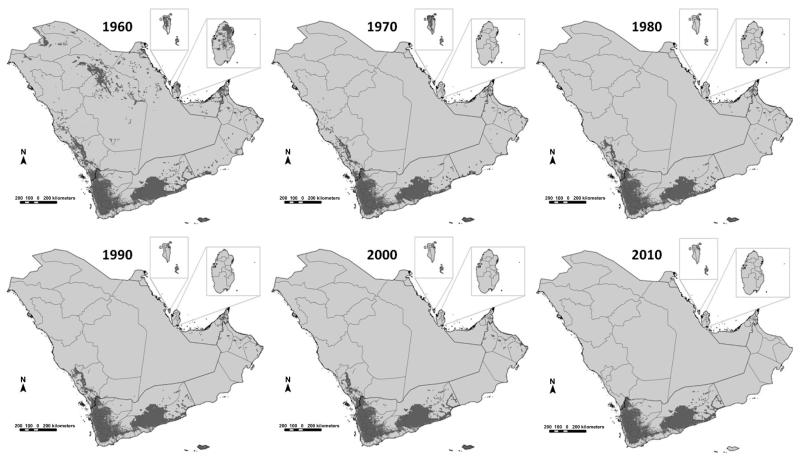
The transmission of malaria across the Arabian Peninsula is governed by the diversity of dominant vectors and extreme aridity. It is likely that where malaria transmission was historically possible it was intense and led to a high disease burden. Here, we review the speed of elimination, approaches taken, define the shrinking map of risk since 1960 and discuss the threats posed to a malaria-free Arabian Peninsula using the archive material, case data and published works. From as early as the 1940s, attempts were made to eliminate malaria on the peninsula but were met with varying degrees of success through to the 1970s; however, these did result in a shrinking of the margins of malaria transmission across the peninsula. Epidemics in the 1990s galvanised national malaria control programmes to reinvigorate control efforts. Before the launch of the recent global ambition for malaria eradication, countries on the Arabian Peninsula launched a collaborative malaria-free initiative in 2005. This initiative led a further shrinking of the malaria risk map and today locally acquired clinical cases of malaria are reported only in Saudi Arabia and Yemen, with the latter contributing to over 98% of the clinical burden.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
References
-
- Abdel-Hameed AA. Antimalarial drug resistance in the Eastern Mediterranean region. East. Mediterr. Health J. 2003;9:492–509. - PubMed
-
- Abdoon AMMO, Alshahrani AM. Prevalence and distribution of Anopheline mosquitoes in malaria endemic areas of Asia region, Saudi Arabia. East. Mediterr. Health J. 2003;9:240–247. - PubMed
-
- Afridi MK, Majid SA. Malaria in Bahrain Islands (Persian Gulf) J. Mal. Inst. India. 1938;1:428–452.
-
- Al Abdullalatif Z, Fontaine RE, Saeed AB, Al Hamdan N, Al Sagheer S. Malaria outbreak in Gellwa, Al Baha, Saudi Arabia, January to March 1996. Saudi Epidemiol. Bull. 1996;3:27–29.
-
- Al Tawfiq JA. Epidemiology of travel-related malaria in a non-malarious area in Saudi Arabia. Saudi Med. J. 2006;27:86–89. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
