

An undiagnosed left sided traumatic diaphragmatic hernia presenting as small intestinal strangulation: A case report
- PMID: 23548705
- PMCID: PMC3731691
- DOI: 10.1016/j.ijscr.2013.02.006
An undiagnosed left sided traumatic diaphragmatic hernia presenting as small intestinal strangulation: A case report
Abstract
Introduction: Post traumatic diaphragmatic hernia is very often missed particularly in polytrauma patients. We present case of an isolated post traumatic diaphragmatic hernia with strangulation, a very rare finding.
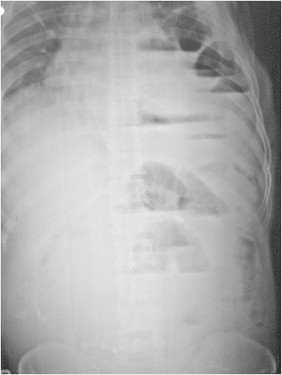
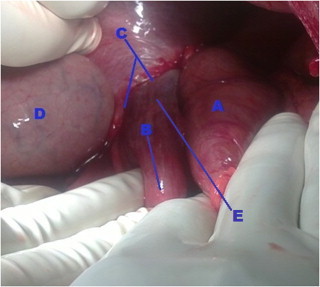
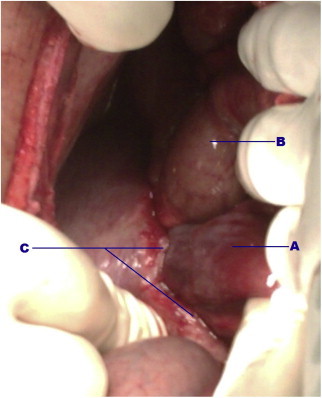
Presentation of case: A 35 year old man presented with features of intestinal obstruction with past history of a seemingly trivial blunt thoracic injury 15 years back. Findings of X-ray abdomen and chest with high leukocyte count raised suspicion of obstructed diaphragmatic hernia which on exploration revealed obstructed diaphragmatic hernia with gangrenous bowel segment.
Discussion: Blunt injury of diaphragm is relatively common and is considered as a marker of severe trauma and it can clinically be occult as other violent injuries may mask and disguise its initial clinical presentation(1) resulting in late presentation with obstruction and/or rarely strangulation. An early diagnosis of the condition is prudent to avoid morbidity and mortality associated with late presentations.
Conclusion: In a patient of intestinal obstruction with history of even trivial throraco- abdominal injury, diagnosis of diaphragmatic hernia should be kept in mind.
Copyright © 2013 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Petrone P., Leppaniemi A., Inaba K., Soreide K., Asensio J.A. Diaphragmatic injuries: challenges in the diagnosis and management. Trauma. 2007;9:227–236.
-
- Jeyarajah R., Harford W.V. Sliesenger and Fordtran's gastrointestinal and liver disease. 8th ed. Saunders, Elsevier; 2006. Abdominal hernias and gastric volvulus. p. 477–81.
-
- Dexter J.R., Gold P.M. Acute onset of dyspnoea associated with colonoscopy. Journal of the American Medical Association. 1980;244:1239–1240. - PubMed
-
- Crandall M., Popowich D., Shapiro M., West M. Posttraumatic hernias: historical overview and review of the literature. The American Surgeon. 2007;73(9):845–850. - PubMed
-
- Yilmaz M., Isik B., Ara C., Yilmaz S., Kutlu R., Kocak O. Gastric perforation during chest tube placement for acute diaphragmatic rupture and review of the literature. Injury Extra. 2006;37:71–75.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
