

Epitope specificity determines pathogenicity and detectability in ANCA-associated vasculitis
- PMID: 23549081
- PMCID: PMC3613913
- DOI: 10.1172/JCI65292
Epitope specificity determines pathogenicity and detectability in ANCA-associated vasculitis
Abstract
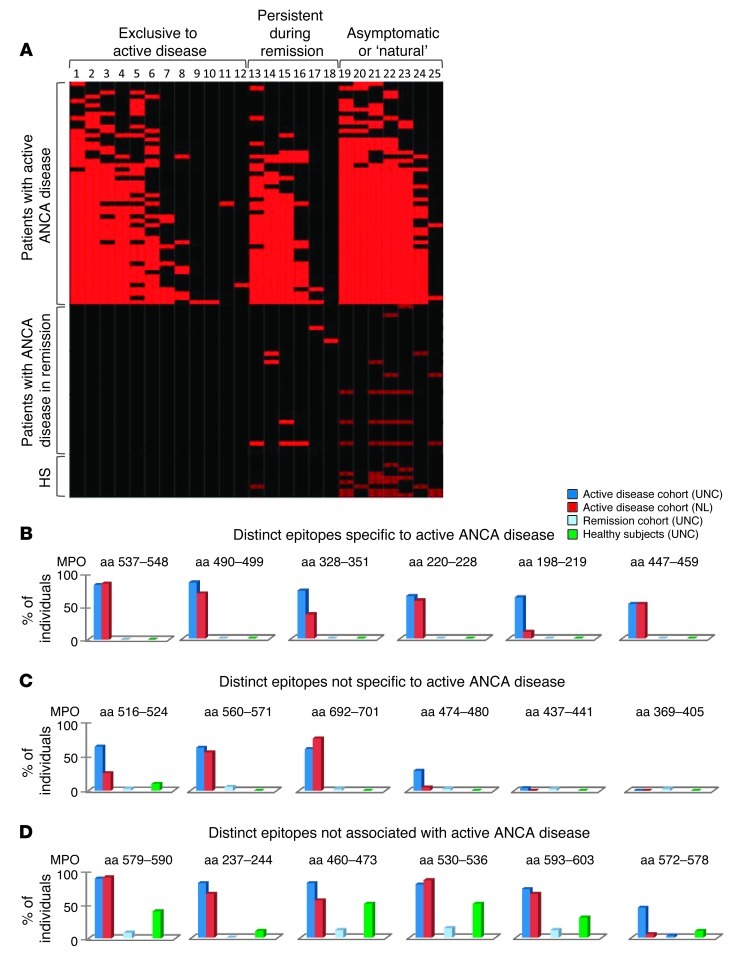
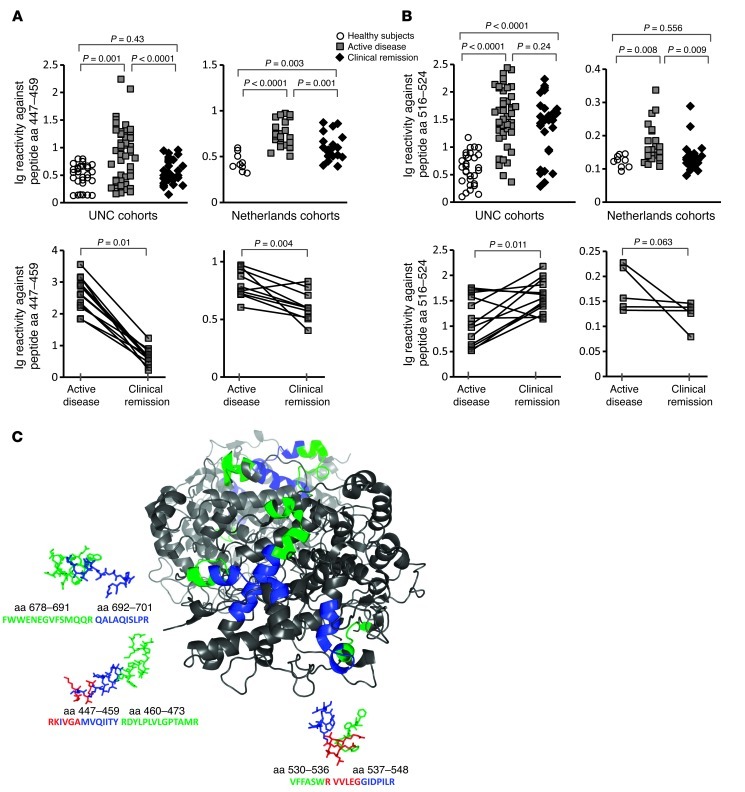
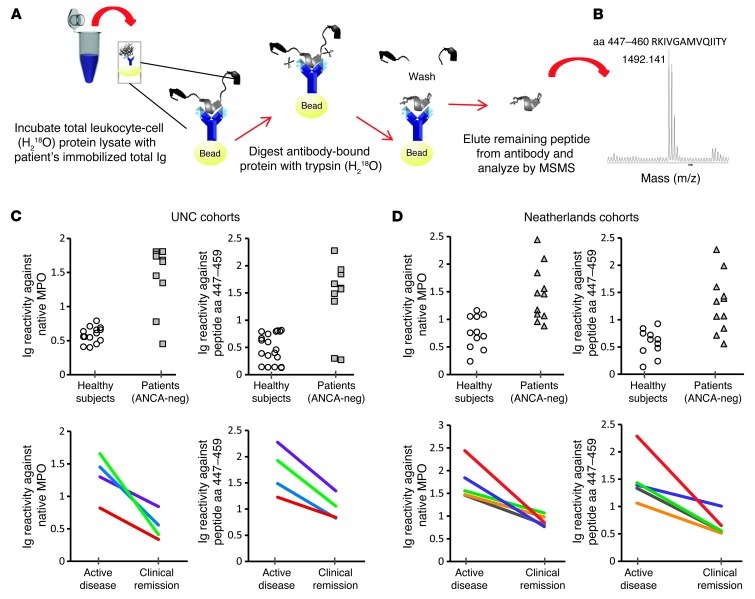
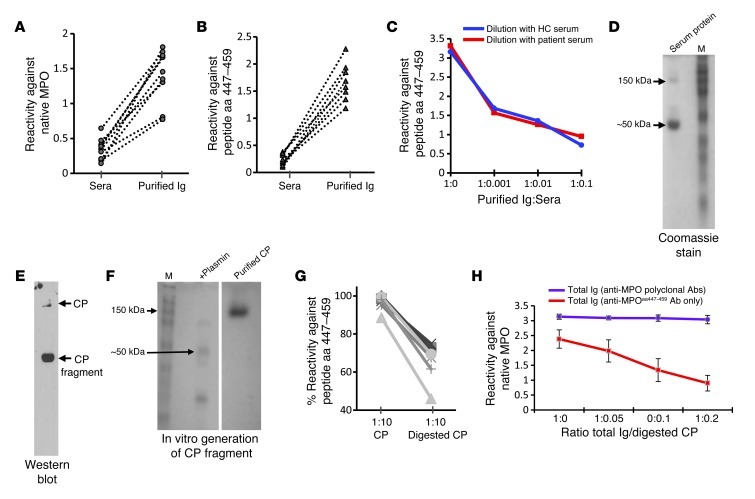
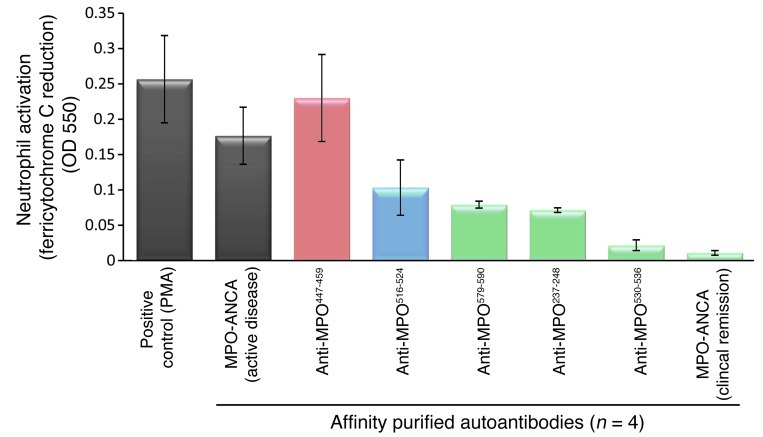
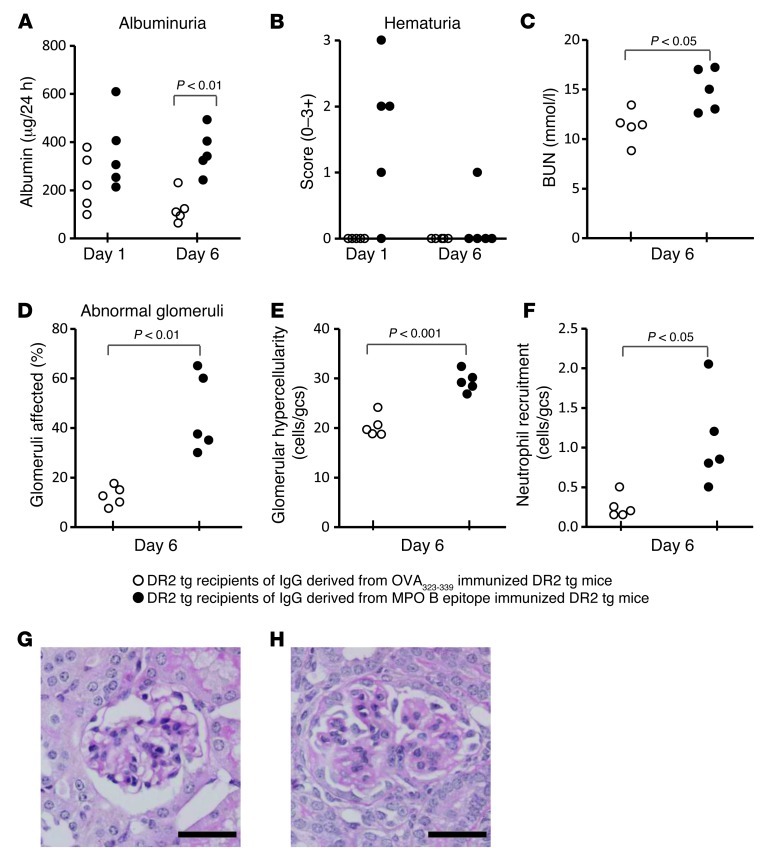
Anti-neutrophil cytoplasmic antibody-associated (ANCA-associated) small vessel necrotizing vasculitis is caused by immune-mediated inflammation of the vessel wall and is diagnosed in some cases by the presence of myeloperoxidase-specific antibodies (MPO-ANCA). This multicenter study sought to determine whether differences in ANCA epitope specificity explain why, in some cases, conventional serologic assays do not correlate with disease activity, why naturally occurring anti-MPO autoantibodies can exist in disease-free individuals, and why ANCA are undetected in patients with ANCA-negative disease. Autoantibodies from human and murine samples were epitope mapped using a highly sensitive epitope excision/mass spectrometry approach. Data indicated that MPO autoantibodies from healthy individuals had epitope specificities different from those present in ANCA disease. Importantly, this methodology led to the discovery of MPO-ANCA in ANCA-negative disease that reacted against a sole linear sequence. Autoantibodies against this epitope had pathogenic properties, as demonstrated by their capacity to activate neutrophils in vitro and to induce nephritis in mice. The confounder for serological detection of these autoantibodies was the presence of a fragment of ceruloplasmin in serum, which was eliminated in purified IgG, allowing detection. These findings implicate immunodominant epitopes in the pathology of ANCA-associated vasculitis and suggest that autoantibody diversity may be common to other autoimmune diseases.
Figures
Comment in
-
Vasculitis: Epitope specificity responsible for MPO-ANCA pathogenicity.Nat Rev Nephrol. 2013 Jun;9(6):310. doi: 10.1038/nrneph.2013.71. Epub 2013 Apr 2. Nat Rev Nephrol. 2013. PMID: 23545589 No abstract available.
References
-
- Tervaert JW, Stegeman CA, Kallenberg CG. Serial ANCA testing is useful in monitoring disease activity of patients with ANCA-associated vasculitides. Sarcoidosis Vasc Diffuse Lung Dis. 1996;13(3):241–245. - PubMed
-
- Hogan SL, Nachman PH, Wilkman AS, Jennette JC, Falk RJ. Prognostic markers in patients with antineutrophil cytoplasmic autoantibody-associated microscopic polyangiitis and glomerulonephritis. J Am Soc Nephrol. 1996;7(1):23–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
