

Clinical prediction model to aid emergency doctors managing febrile children at risk of serious bacterial infections: diagnostic study
- PMID: 23550046
- PMCID: PMC3614186
- DOI: 10.1136/bmj.f1706
Clinical prediction model to aid emergency doctors managing febrile children at risk of serious bacterial infections: diagnostic study
Abstract
Objective: To derive, cross validate, and externally validate a clinical prediction model that assesses the risks of different serious bacterial infections in children with fever at the emergency department.
Design: Prospective observational diagnostic study.
Setting: Three paediatric emergency care units: two in the Netherlands and one in the United Kingdom.
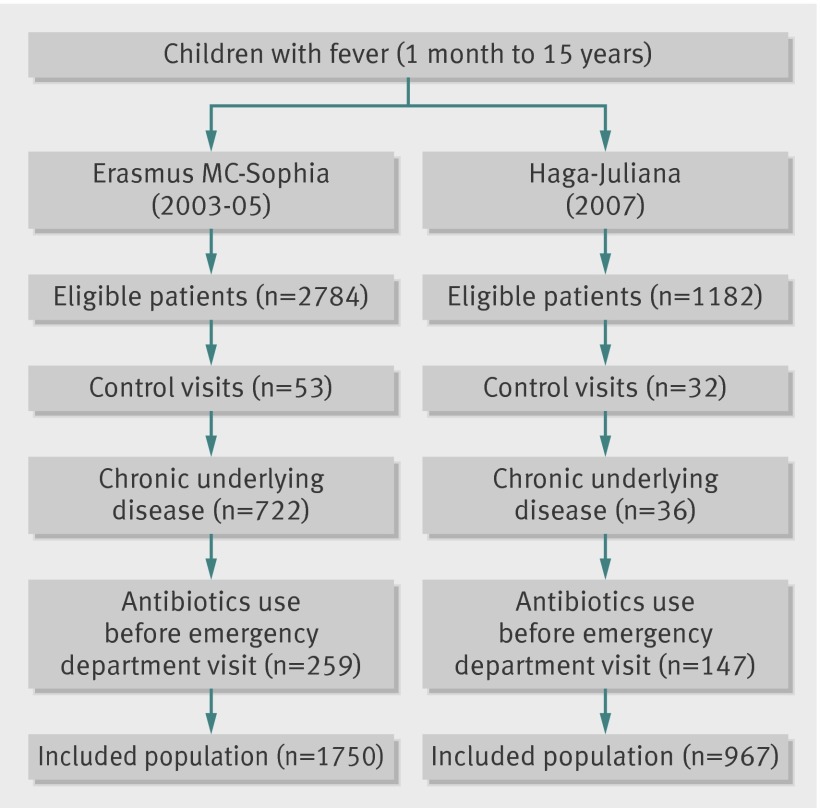
Participants: Children with fever, aged 1 month to 15 years, at three paediatric emergency care units: Rotterdam (n=1750) and the Hague (n=967), the Netherlands, and Coventry (n=487), United Kingdom. A prediction model was constructed using multivariable polytomous logistic regression analysis and included the predefined predictor variables age, duration of fever, tachycardia, temperature, tachypnoea, ill appearance, chest wall retractions, prolonged capillary refill time (>3 seconds), oxygen saturation <94%, and C reactive protein.
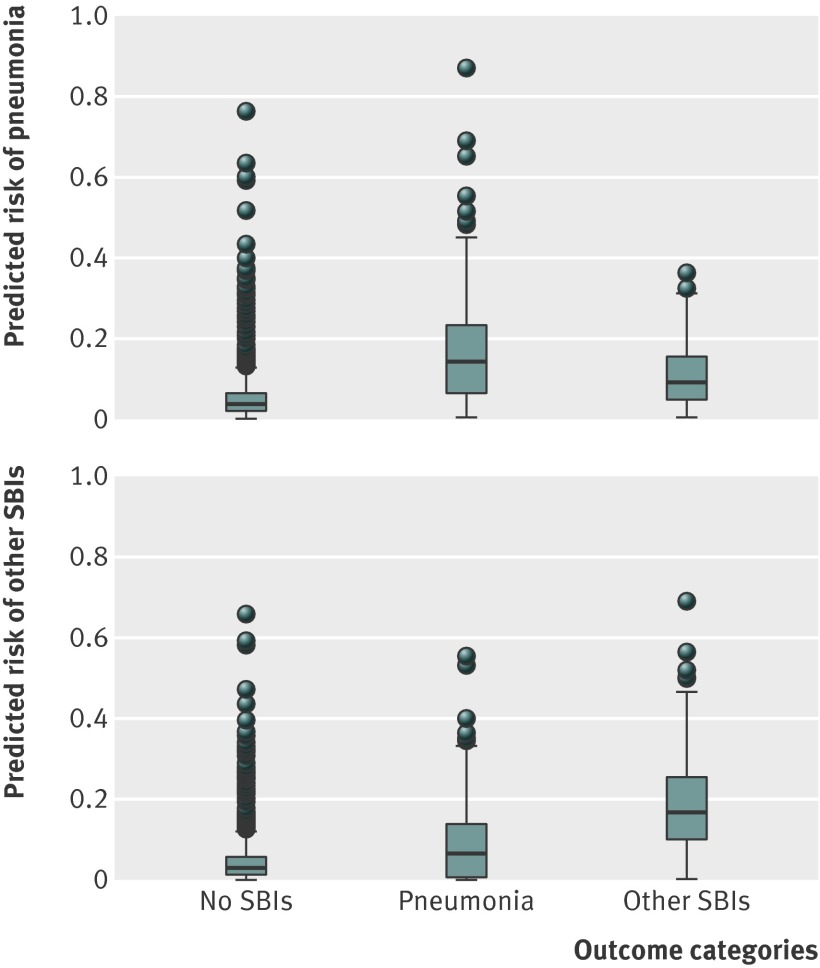
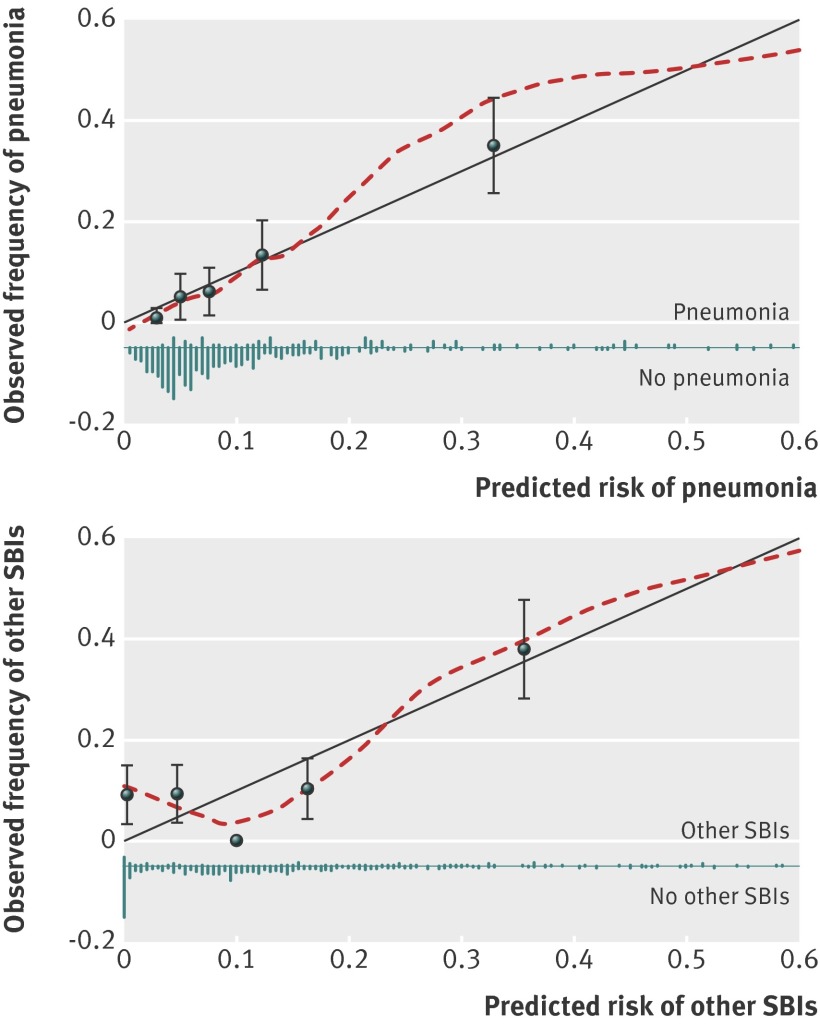
Main outcome measures: Pneumonia, other serious bacterial infections (SBIs, including septicaemia/meningitis, urinary tract infections, and others), and no SBIs.
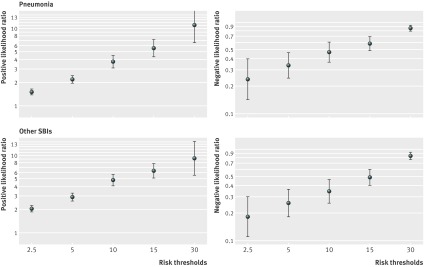
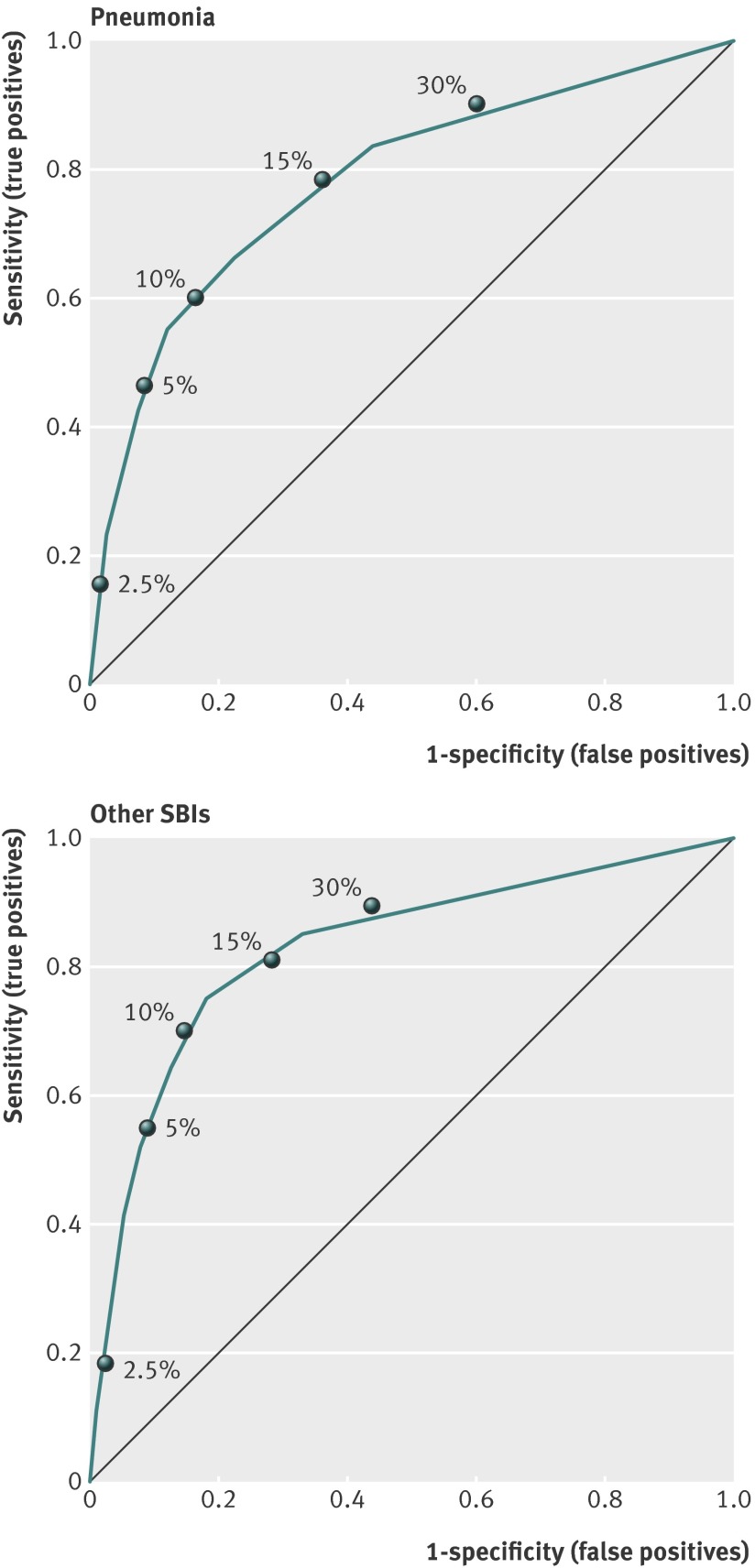
Results: Oxygen saturation <94% and presence of tachypnoea were important predictors of pneumonia. A raised C reactive protein level predicted the presence of both pneumonia and other SBIs, whereas chest wall retractions and oxygen saturation <94% were useful to rule out the presence of other SBIs. Discriminative ability (C statistic) to predict pneumonia was 0.81 (95% confidence interval 0.73 to 0.88); for other SBIs this was even better: 0.86 (0.79 to 0.92). Risk thresholds of 10% or more were useful to identify children with serious bacterial infections; risk thresholds less than 2.5% were useful to rule out the presence of serious bacterial infections. External validation showed good discrimination for the prediction of pneumonia (0.81, 0.69 to 0.93); discriminative ability for the prediction of other SBIs was lower (0.69, 0.53 to 0.86).
Conclusion: A validated prediction model, including clinical signs, symptoms, and C reactive protein level, was useful for estimating the likelihood of pneumonia and other SBIs in children with fever, such as septicaemia/meningitis and urinary tract infections.
Conflict of interest statement
Competing interest: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Kuppermann N, Fleisher GR, Jaffe DM. Predictors of occult pneumococcal bacteremia in young febrile children. Ann Emerg Med 1998;31:679-87. - PubMed
-
- Nelson DS, Walsh K, Fleisher GR. Spectrum and frequency of pediatric illness presenting to a general community hospital emergency department. Pediatrics 1992;90:5-10. - PubMed
-
- Slater M, Krug SE. Evaluation of the infant with fever without source: an evidence based approach. Emerg Med Clin North Am 1999;17:97-126, viii-ix. - PubMed
-
- Neuman MI, Monuteaux MC, Scully KJ, Bachur RG. Prediction of pneumonia in a pediatric emergency department. Pediatrics 2011;128:246-53. - PubMed
-
- Bleeker SE, Derksen-Lubsen G, Grobbee DE, Donders AR, Moons KG, Moll HA. Validating and updating a prediction rule for serious bacterial infection in patients with fever without source. Acta Paediatr 2007;96:100-4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials