

Combination antifungal therapy for cryptococcal meningitis
- PMID: 23550668
- PMCID: PMC3978204
- DOI: 10.1056/NEJMoa1110404
Combination antifungal therapy for cryptococcal meningitis
Abstract
Background: Combination antifungal therapy (amphotericin B deoxycholate and flucytosine) is the recommended treatment for cryptococcal meningitis but has not been shown to reduce mortality, as compared with amphotericin B alone. We performed a randomized, controlled trial to determine whether combining flucytosine or high-dose fluconazole with high-dose amphotericin B improved survival at 14 and 70 days.
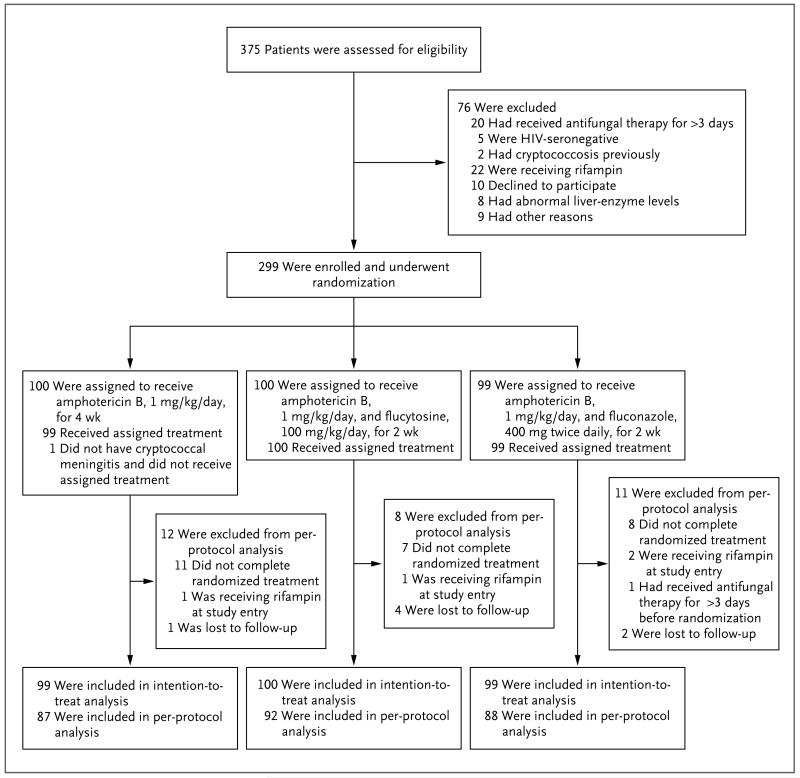
Methods: We conducted a randomized, three-group, open-label trial of induction therapy for cryptococcal meningitis in patients with human immunodeficiency virus infection. All patients received amphotericin B at a dose of 1 mg per kilogram of body weight per day; patients in group 1 were treated for 4 weeks, and those in groups 2 and 3 for 2 weeks. Patients in group 2 concurrently received flucytosine at a dose of 100 mg per kilogram per day for 2 weeks, and those in group 3 concurrently received fluconazole at a dose of 400 mg twice daily for 2 weeks.
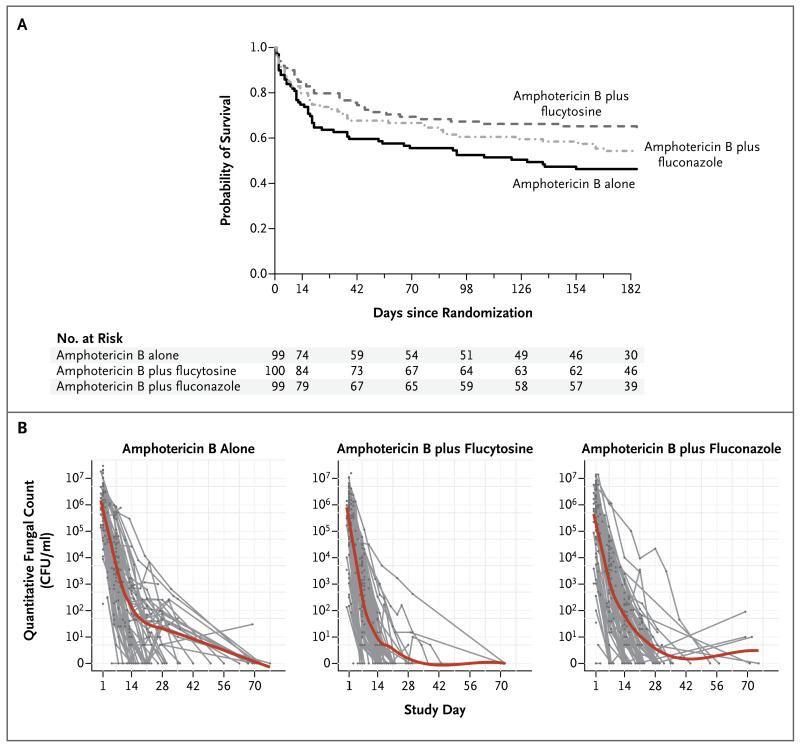
Results: A total of 299 patients were enrolled. Fewer deaths occurred by days 14 and 70 among patients receiving amphotericin B and flucytosine than among those receiving amphotericin B alone (15 vs. 25 deaths by day 14; hazard ratio, 0.57; 95% confidence interval [CI], 0.30 to 1.08; unadjusted P=0.08; and 30 vs. 44 deaths by day 70; hazard ratio, 0.61; 95% CI, 0.39 to 0.97; unadjusted P=0.04). Combination therapy with fluconazole had no significant effect on survival, as compared with monotherapy (hazard ratio for death by 14 days, 0.78; 95% CI, 0.44 to 1.41; P=0.42; hazard ratio for death by 70 days, 0.71; 95% CI, 0.45 to 1.11; P=0.13). Amphotericin B plus flucytosine was associated with significantly increased rates of yeast clearance from cerebrospinal fluid (-0.42 log10 colony-forming units [CFU] per milliliter per day vs. -0.31 and -0.32 log10 CFU per milliliter per day in groups 1 and 3, respectively; P<0.001 for both comparisons). Rates of adverse events were similar in all groups, although neutropenia was more frequent in patients receiving a combination therapy.
Conclusions: Amphotericin B plus flucytosine, as compared with amphotericin B alone, is associated with improved survival among patients with cryptococcal meningitis. A survival benefit of amphotericin B plus fluconazole was not found. (Funded by the Wellcome Trust and the British Infection Society; Controlled-Trials.com number, ISRCTN95123928.).
Figures
Comment in
-
Efficiently killing a sugar-coated yeast.N Engl J Med. 2013 Apr 4;368(14):1354-6. doi: 10.1056/NEJMe1302038. N Engl J Med. 2013. PMID: 23550675 No abstract available.
-
Combination antifungal therapy for cryptococcal meningitis.N Engl J Med. 2013 Jun 27;368(26):2522-3. doi: 10.1056/NEJMc1305981. N Engl J Med. 2013. PMID: 23802521 No abstract available.
-
Combination antifungal therapy for cryptococcal meningitis.N Engl J Med. 2013 Jun 27;368(26):2522. doi: 10.1056/NEJMc1305981. N Engl J Med. 2013. PMID: 23802522 No abstract available.
References
-
- Park BJ, Wannemuehler KA, Marston BJ, Govender N, Pappas PG, Chiller TM. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS. 2009;23:525–30. - PubMed
-
- van der Horst CM, Saag MS, Cloud GA, et al. Treatment of cryptococcal meningitis associated with the acquired immunodeficiency syndrome. N Engl J Med. 1997;337:15–21. - PubMed
-
- Sloan D, Dlamini S, Paul N, Dedicoat M. Treatment of acute cryptococcal meningitis in HIV infected adults, with an emphasis on resource-limited settings. Cochrane Database Syst Rev. 2008;4:CD005647. - PubMed
-
- Brouwer AE, Rajanuwong A, Chierakul W, et al. Combination antifungal therapies for HIV-associated cryptococcal meningitis: a randomised trial. Lancet. 2004;363:1764–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical