

Enteral vs. intravenous ICU sedation management: study protocol for a randomized controlled trial
- PMID: 23551983
- PMCID: PMC3651718
- DOI: 10.1186/1745-6215-14-92
Enteral vs. intravenous ICU sedation management: study protocol for a randomized controlled trial
Abstract
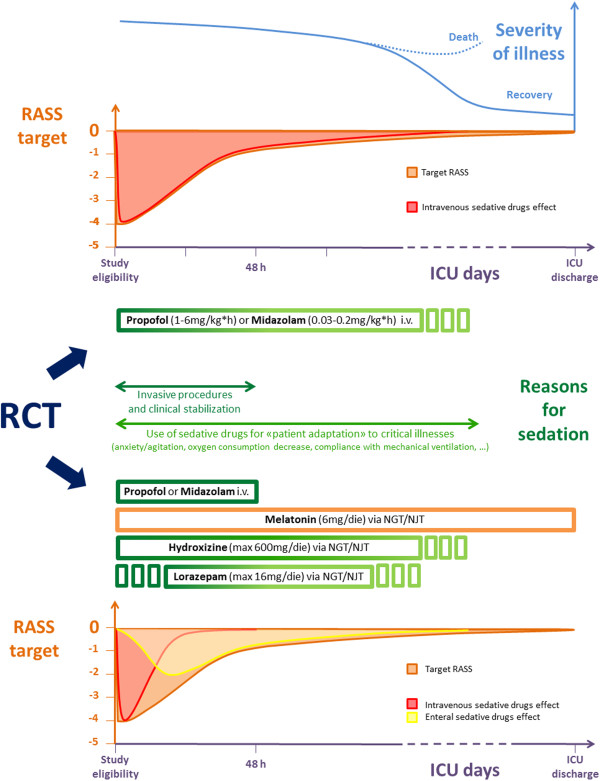
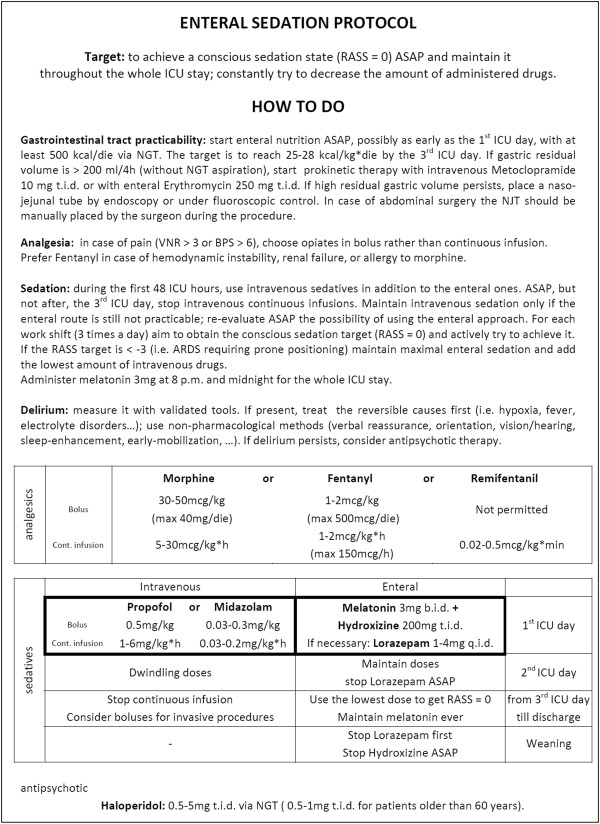
Background: A relevant innovation about sedation of long-term Intensive Care Unit (ICU) patients is the 'conscious target': patients should be awake even during the critical phases of illness. Enteral sedative administration is nowadays unusual, even though the gastrointestinal tract works soon after ICU admission. The enteral approach cannot produce deep sedation; however, it is as adequate as the intravenous one, if the target is to keep patients awake and adapted to the environment, and has fewer side effects and lower costs.
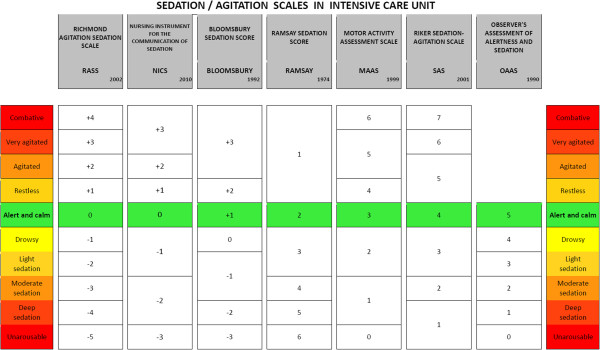
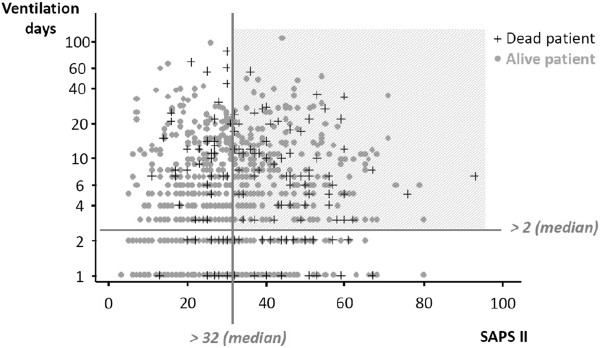
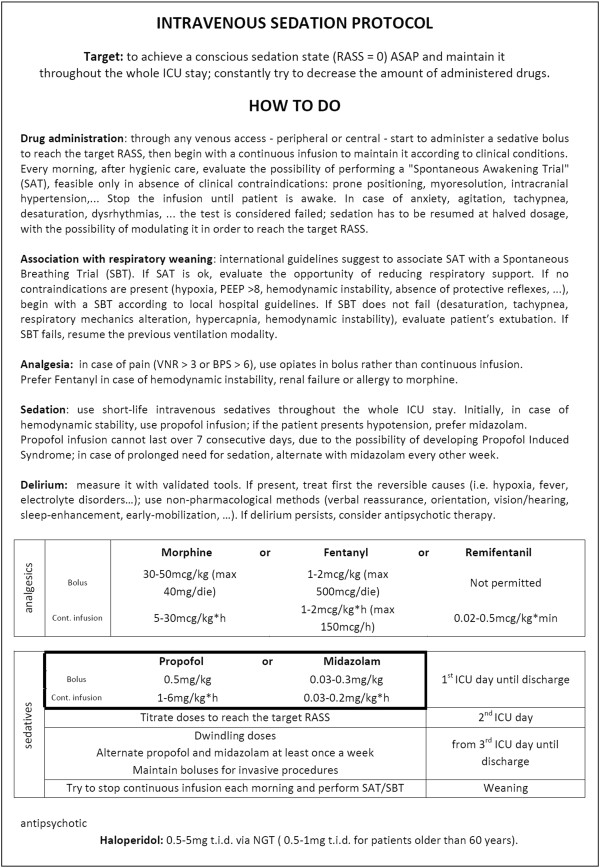
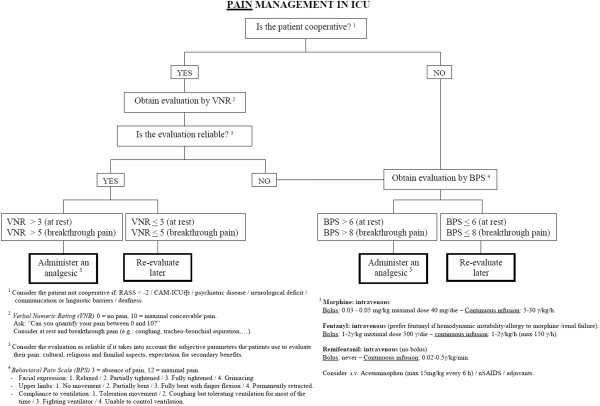
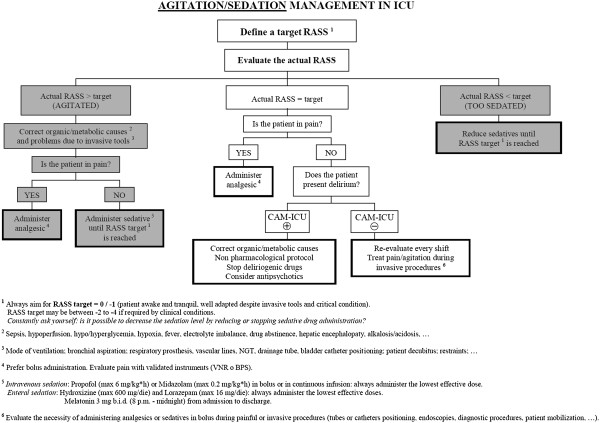
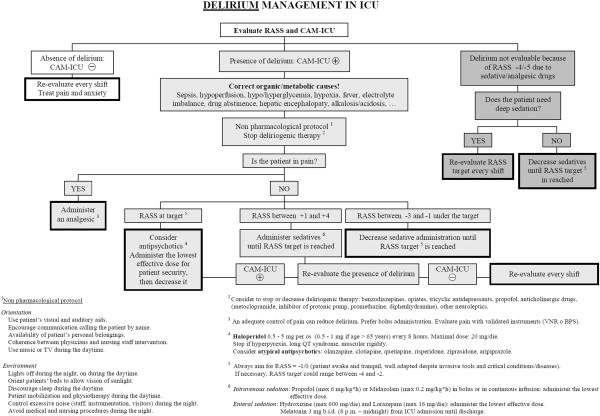
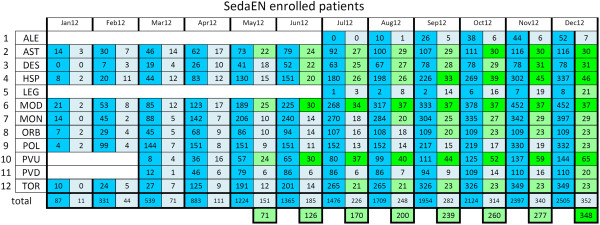
Methods/design: A randomized, controlled, multicenter, single-blind trial comparing enteral and intravenous sedative treatments has been done in 12 Italian ICUs. The main objective was to achieve and maintain the desired sedation level: observed RASS = target RASS ± 1. Three hundred high-risk patients were planned to be randomly assigned to receive either intravenous propofol/midazolam or enteral melatonin/hydroxyzine/lorazepam. Group assignment occurred through online minimization process, in order to balance variables potentially influencing the outcomes (age, sex, SAPS II, type of admission, kidney failure, chronic obstructive pulmonary disease, sepsis) between groups. Once per shift, the staff recorded neurological monitoring using validated tools. Three flowcharts for pain, sedation, and delirium have been proposed; they have been designed to treat potentially correctable factors first, and, only once excluded, to administer neuroactive drugs. The study lasted from January 24 to December 31, 2012. A total of 348 patients have been randomized, through a centralized website, using a specific software expressly designed for this study. The created network of ICUs included a mix of both university and non-university hospitals, with different experience in managing enteral sedation. A dedicated free-access website was also created, in both Italian and English, for continuous education of ICU staff through CME courses.
Discussion: This 'educational research' project aims both to compare two sedative strategies and to highlight the need for a profound cultural change, improving outcomes by keeping critically-ill patients awake.
Trial registration number: Clinicaltrials.gov #NCT01360346.
Figures

References
-
- Martin J, Heymann A, Basell K, Baron R, Biniek R, Burkle H, Dall P, Dictus C, Eggers V, Eichler I, Engelmann L, Garten L, Hartl W, Haase U, Huth R, Kessler P, Kleinschmidt S, Koppert W, Kretz FJ, Laubenthal H, Marggraf G, Meiser A, Neugebauer E, Neuhaus U, Putensen C, Quintel M, Reske A, Roth B, Scholz J, Schroder S. Evidence and consensus-based German guidelines for the management of analgesia, sedation and delirium in intensive care–short version. Ger Med Sci. 2010;8:Doc02. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
