

Cost-effectiveness analysis of Option B+ for HIV prevention and treatment of mothers and children in Malawi
- PMID: 23554867
- PMCID: PMC3595266
- DOI: 10.1371/journal.pone.0057778
Cost-effectiveness analysis of Option B+ for HIV prevention and treatment of mothers and children in Malawi
Abstract
Background: The Ministry of Health in Malawi is implementing a pragmatic and innovative approach for the management of all HIV-infected pregnant women, termed Option B+, which consists of providing life-long antiretroviral treatment, regardless of their CD4 count or clinical stage. Our objective was to determine if Option B+ represents a cost-effective option.
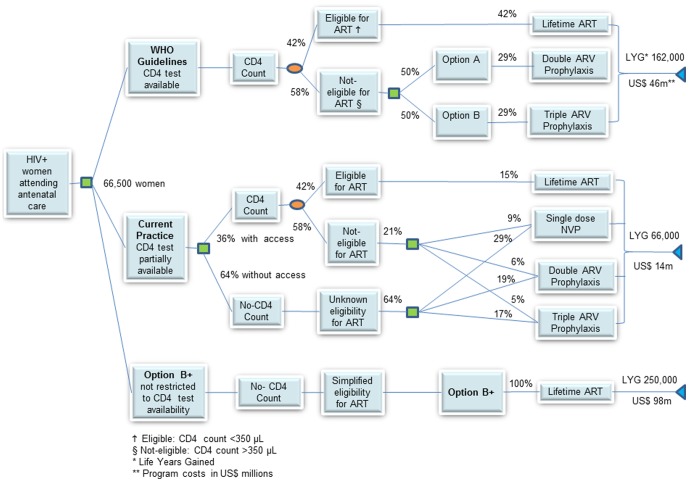
Methods: A decision model simulates the disease progression of a cohort of HIV-infected pregnant women receiving prophylaxis and antiretroviral therapy, and estimates the number of paediatric infections averted and maternal life years gained over a ten-year time horizon. We assess the cost-effectiveness from the Ministry of Health perspective while taking into account the practical realities of implementing ART services in Malawi.
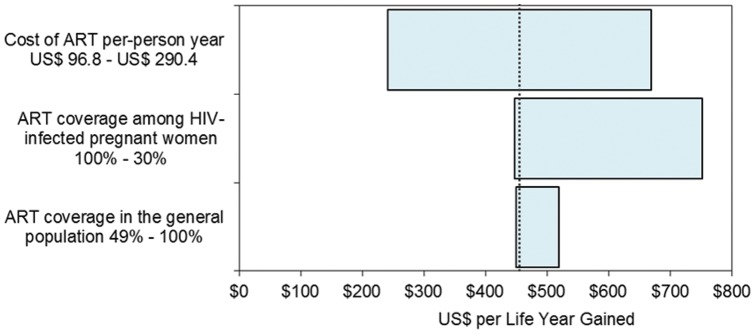
Results: If implemented as recommended by the World Health Organization, options A, B and B+ are equivalent in preventing new infant infections, yielding cost effectiveness ratios between US$ 37 and US$ 69 per disability adjusted life year averted in children. However, when the three options are compared to the current practice, the provision of antiretroviral therapy to all mothers (Option B+) not only prevents infant infections, but also improves the ten-year survival in mothers more than four-fold. This translates into saving more than 250,000 maternal life years, as compared to mothers receiving only Option A or B, with savings of 153,000 and 172,000 life years respectively. Option B+ also yields favourable incremental cost effectiveness ratios (ICER) of US$ 455 per life year gained over the current practice.
Conclusion: In Malawi, Option B+ represents a favorable policy option from a cost-effectiveness perspective to prevent future infant infections, save mothers' lives and reduce orphanhood. Although Option B+ would require more financial resources initially, it would save societal resources in the long-term and represents a strategic option to simplify and integrate HIV services into maternal, newborn and child health programmes.
Conflict of interest statement
Figures

References
-
- UNAIDS (2011) Outlook Report: 30 years into the AIDS epidemic. Available: http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspubl....Accessed 2013 Feb 2.
-
- WHO UNAIDS, UNICEF (2011) Global HIV/AIDS Response. Epidemic update and health sector progress towards Universal Access. Available: www.who.int/hiv/pub/progress_report2011/en/index.html.Accessed 2011 Nov 30.
-
- Townsend CL, Cortina-Borja M, Peckham CS, de Ruiter A, Lyall H, at al (2008) Low rates of mother-to-child transmission of HIV following effective pregnancy interventions in the United Kingdom and Ireland, 2000–2006. AIDS 22: 973–981. - PubMed
-
- McKenna MT, Hu XH (2007) Recent trends in the incidence and morbidity that are associated with perinatal human immunodeficiency virus infection in the United States. Am J Obstet Gynecol 197: S10–S16. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
