

Prevalence of symptomatic heart failure with reduced and with normal ejection fraction in an elderly general population-the CARLA study
- PMID: 23555000
- PMCID: PMC3598658
- DOI: 10.1371/journal.pone.0059225
Prevalence of symptomatic heart failure with reduced and with normal ejection fraction in an elderly general population-the CARLA study
Abstract
Background/objectives: Chronic heart failure (CHF) is one of the most important public health concerns in the industrialized world having increasing incidence and prevalence. Although there are several studies describing the prevalence of heart failure with reduced ejection fraction (HFREF) and heart failure with normal ejection fraction (HFNEF) in selected populations, there are few data regarding the prevalence and the determinants of symptomatic heart failure in the general population.
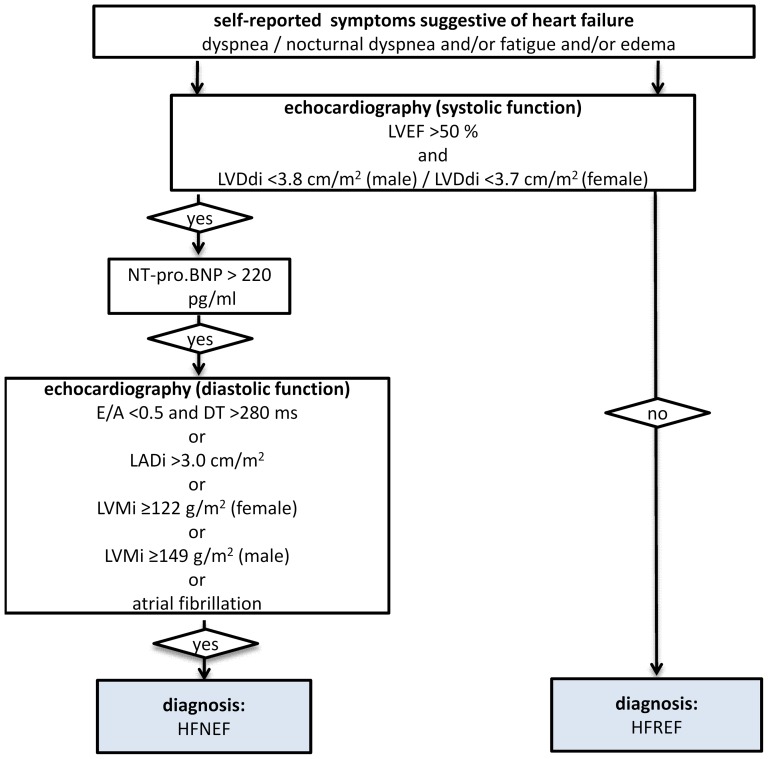
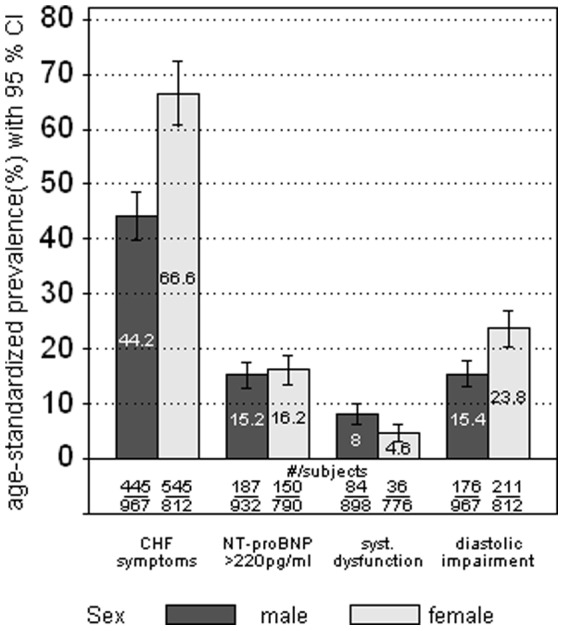
Methods: Cross-sectional data of a population-based German sample (1,779 subjects aged 45-83 years) were analyzed to determine the prevalence and determinants of chronic SHF and HFNEF defined according to the European Society of Cardiology using symptoms, echocardiography and serum NT-proBNP. Prevalence was age-standardized to the German population as of December 31st, 2005.
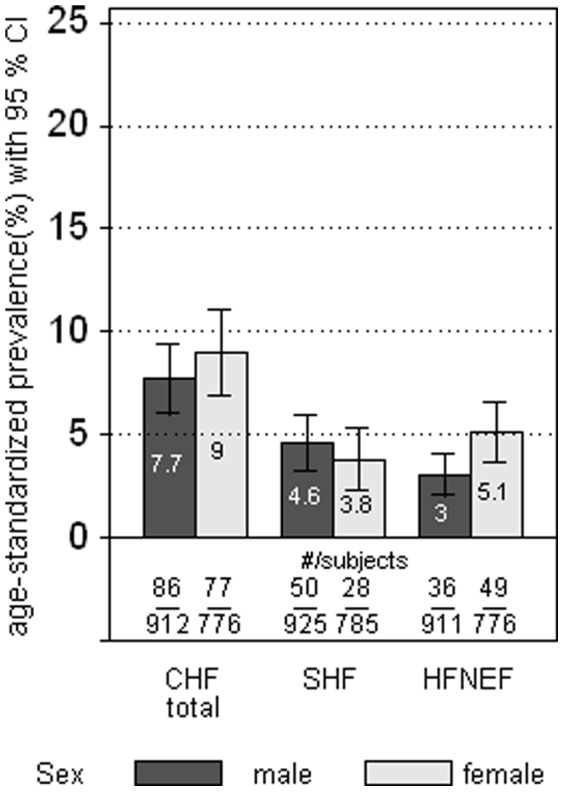
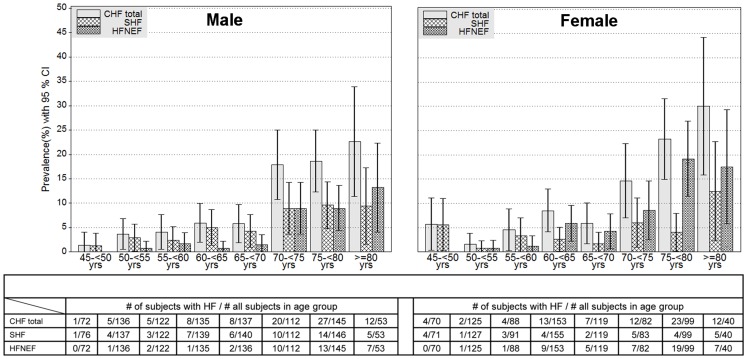
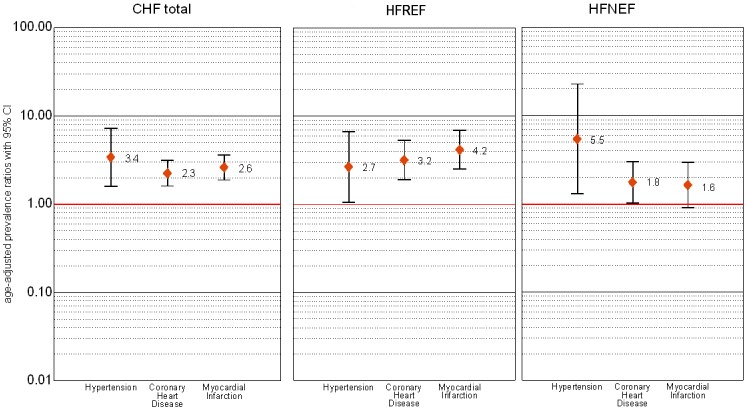
Results: The overall age-standardized prevalence of symptomatic CHF was 7.7% (95%CI 6.0-9.8) for men and 9.0% (95%CI 7.0-11.5) for women. The prevalence of CHF strongly increased with age from 3.0% among 45-54- year-old subjects to 22.0% among 75-83- year-old subjects. Symptomatic HFREF could be shown in 48% (n = 78), symptomatic HFNEF in 52% (n = 85) of subjects with CHF. The age-standardized prevalence of HFREF was 3.8 % (95%CI 2.4-5.8) for women and 4.6 % (95%CI 3.6-6.3) for men. The age-standardized prevalence of HFNEF for women and men was 5.1 % (95%CI 3.8-7.0) and 3.0 % (95%CI 2.1-4.5), respectively. Persons with CHF were more likely to have hypertension (PR = 3.4; 95%CI 1.6-7.3) or to have had a previous myocardial infarction (PR = 2.5, 95%CI 1.8-3.5).
Conclusion: The prevalence of symptomatic CHF appears high in this population compared with other studies. While more women were affected by HFNEF than men, more male subjects suffered from HFREF. The high prevalence of symptomatic CHF seems likely to be mainly due to the high prevalence of cardiovascular risk factors in this population.
Conflict of interest statement
Figures
Similar articles
-
Prevalence, Presentation, and Outcome of Heart Failure with Preserved Ejection Fraction among Patients Presenting with Undifferentiated Dyspnoea to the Emergency Room: A 10-year Analysis from a Tertiary Centre.Ann Acad Med Singap. 2016 Jan;45(1):18-26. Ann Acad Med Singap. 2016. PMID: 27118225
-
The level of NT-proBNP in ambulatory patients with chronic heart failure with preserved ejection fraction of the left ventricle.Ter Arkh. 2018 Sep 20;90(9):68-72. doi: 10.26442/terarkh201890968-72. Ter Arkh. 2018. PMID: 30701738
-
The role of exercise echocardiography in the diagnostics of heart failure with normal left ventricular ejection fraction.Eur J Echocardiogr. 2011 Aug;12(8):591-602. doi: 10.1093/ejechocard/jer082. Epub 2011 Jun 17. Eur J Echocardiogr. 2011. PMID: 21685198
-
Prognosis and NT-proBNP in heart failure patients with preserved versus reduced ejection fraction.Heart. 2019 Aug;105(15):1182-1189. doi: 10.1136/heartjnl-2018-314173. Epub 2019 Apr 8. Heart. 2019. PMID: 30962192 Free PMC article.
-
Heart failure with normal ejection fraction: new diagnostic criteria and pathophysiological advances.Arq Bras Cardiol. 2009 Aug;93(2):180-7. doi: 10.1590/s0066-782x2009000800018. Arq Bras Cardiol. 2009. PMID: 19838497 Review.
Cited by
-
Sacubitril/Valsartan (LCZ696): A Novel Treatment for Heart Failure and its Estimated Cost Effectiveness, Budget Impact, and Disease Burden Reduction in Germany.Pharmacoeconomics. 2018 Oct;36(10):1285-1296. doi: 10.1007/s40273-018-0688-4. Pharmacoeconomics. 2018. PMID: 30054868
-
Comorbidity of heart failure and chronic obstructive pulmonary disease: more than coincidence.Curr Heart Fail Rep. 2014 Sep;11(3):337-46. doi: 10.1007/s11897-014-0212-x. Curr Heart Fail Rep. 2014. PMID: 24980212 Review.
-
Prevalence and Risk Factors of Heart Failure with Preserved Ejection Fraction: A Population-Based Study in Northeast China.Int J Environ Res Public Health. 2016 Jul 29;13(8):770. doi: 10.3390/ijerph13080770. Int J Environ Res Public Health. 2016. PMID: 27483300 Free PMC article.
-
Performance of Sokolow-Lyon index in detection of echocardiographically diagnosed left ventricular hypertrophy in a normal Eastern German population - results of the CARLA study.BMC Cardiovasc Disord. 2015 Jul 14;15:69. doi: 10.1186/s12872-015-0066-5. BMC Cardiovasc Disord. 2015. PMID: 26169782 Free PMC article.
-
Patients with Heart Failure During and After Inpatient Cardiac Rehabilitation.Vasc Health Risk Manag. 2021 Feb 16;17:49-58. doi: 10.2147/VHRM.S276465. eCollection 2021. Vasc Health Risk Manag. 2021. PMID: 33623387 Free PMC article.
References
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, et al. (2002) Long-term trends in the incidence of and survival with heart failure. N Engl J Med 347: 1397–402. - PubMed
-
- Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJV, Ponikowski P, et al. (2008) ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008 The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur J Heart Fail 10: 933–989. - PubMed
-
- Luchner A, Burnett JC, Jougasaki M, Hense HW, Heid IM, et al. (2000) Evaluation of brain natriuretic peptide as marker of left ventricular dysfunction and hypertrophy in the population. J of Hypertens 18: 1121–1128. - PubMed
-
- Goetze JP, Mogelvang R, Maage L, Scharling H, Schnohr P, et al. (2006) Plasma pro-B-type natriuretic peptide in the general population: screening for left ventricular hypertrophy and systolic dysfunction. Eur Heart J 27: 3004–3010. - PubMed
-
- Vasan RS, Benjamin EJ, Levy D (1995) Prevalence, clinical features and prognosis of diastolic heart failure: an epidemiologic perspective. J Am Coll Cardiol 26: 1565–1574. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
