

Benign hepatocellular tumors in children: focal nodular hyperplasia and hepatocellular adenoma
- PMID: 23555058
- PMCID: PMC3608344
- DOI: 10.1155/2013/215064
Benign hepatocellular tumors in children: focal nodular hyperplasia and hepatocellular adenoma
Abstract
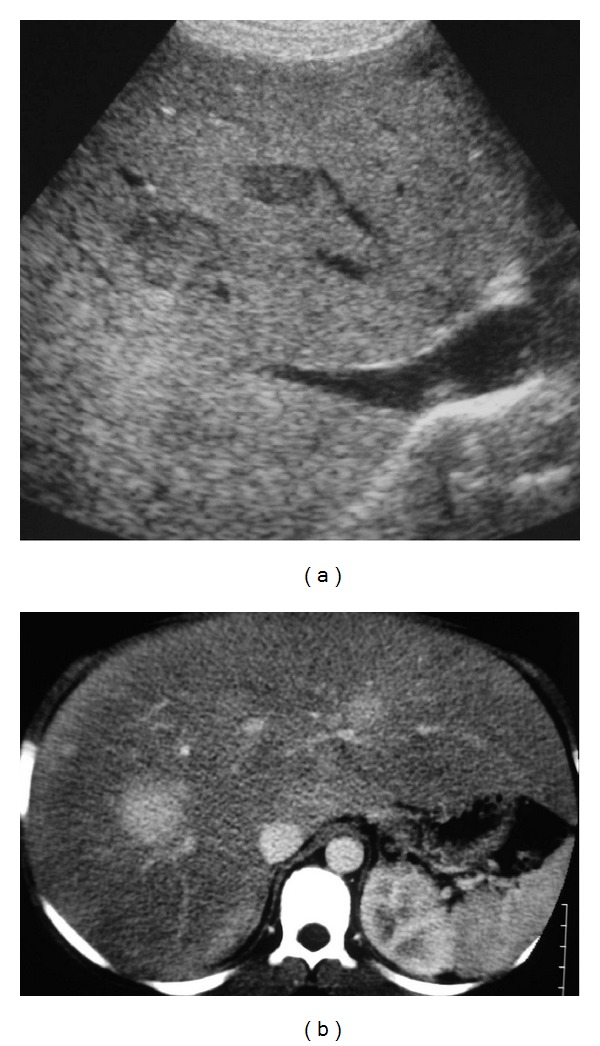
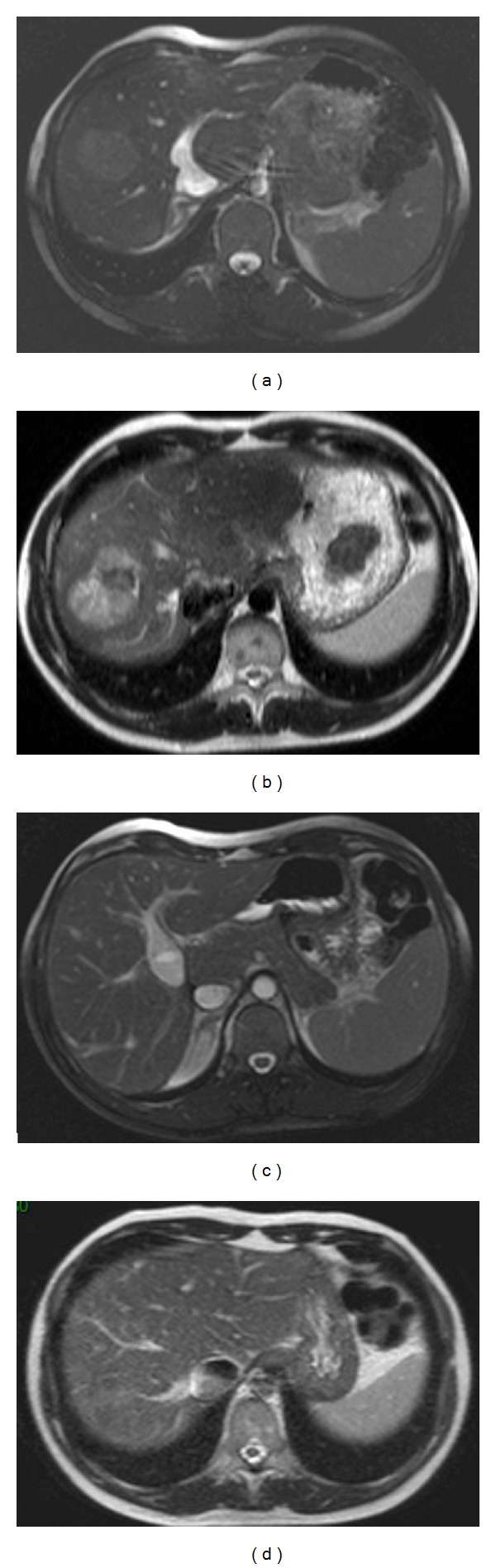
Benign liver tumors are very rare in children. Most focal nodular hyperplasia (FNH) remain sporadic, but predisposing factors exist, as follows: long-term cancer survivor (with an increasing incidence), portal deprivation in congenital or surgical portosystemic shunt. The aspect is atypical on imaging in two-thirds of cases. Biopsy of the tumor and the nontumoral liver is then required. Surgical resection will be discussed in the case of large tumors with or without symptoms. In the case of associated vascular disorder with portal deprivation, restoration of the portal flow will be discussed in the hope of seeing the involution of FNH. HepatoCellular Adenoma (HCA) is frequently associated with predisposing factors such as GSD type I and III, Fanconi anemia especially if androgen therapy is administered, CPSS, and SPSS. Adenomatosis has been reported in germline mutation of HNF1- α . Management will depend on the presence of a predisposing factor and may include metabolic control, androgen therapy withdrawn, or closure of the shunt when appropriate. Surgery is usually performed on large lesions. In the case of adenomatosis or multiple lesions, surgery will be adapted. Close followup is required in all cases.
Figures
References
-
- Fukukura Y, Nakashima O, Kusaba A, Kage M, Kojiro M. Angioarchitecture and blood circulation in focal nodular hyperplasia of the liver. Journal of Hepatology. 1998;29(3):470–475. - PubMed
-
- Wanless IR, Mawdsley C, Adams R. On the pathogenesis of focal nodular hyperplasia of the liver. Hepatology. 1985;5(6):1194–1200. - PubMed
-
- Rebouissou S, Bioulac-Sage P, Zucman-Rossi J. Molecular pathogenesis of focal nodular hyperplasia and hepatocellular adenoma. Journal of Hepatology. 2008;48(1):163–170. - PubMed
-
- Nguyen BN, Fléjou JF, Terris B, Belghiti J, Degott C. Focal nodular hyperplasia of the liver: a comprehensive pathologic study of 305 lesions and recognition of new histologic forms. American Journal of Surgical Pathology. 1999;23(12):1441–1454. - PubMed
-
- Kumagai H, Masuda T, Oikawa H, Endo K, Endo M, Takano T. Focal nodular hyperplasia of the liver: direct evidence of circulatory disturbances. Journal of Gastroenterology and Hepatology. 2000;15(11):1344–1347. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
