

Implementation of high resolution whole genome array CGH in the prenatal clinical setting: advantages, challenges, and review of the literature
- PMID: 23555083
- PMCID: PMC3603644
- DOI: 10.1155/2013/346762
Implementation of high resolution whole genome array CGH in the prenatal clinical setting: advantages, challenges, and review of the literature
Abstract
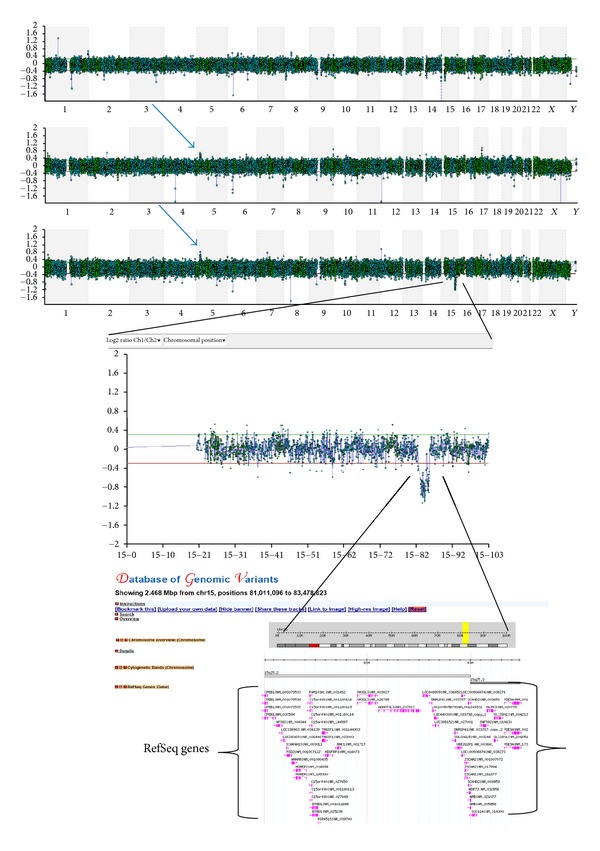
Array Comparative Genomic Hybridization analysis is replacing postnatal chromosomal analysis in cases of intellectual disabilities, and it has been postulated that it might also become the first-tier test in prenatal diagnosis. In this study, array CGH was applied in 64 prenatal samples with whole genome oligonucleotide arrays (BlueGnome, Ltd.) on DNA extracted from chorionic villi, amniotic fluid, foetal blood, and skin samples. Results were confirmed with Fluorescence In Situ Hybridization or Real-Time PCR. Fifty-three cases had normal karyotype and abnormal ultrasound findings, and seven samples had balanced rearrangements, five of which also had ultrasound findings. The value of array CGH in the characterization of previously known aberrations in five samples is also presented. Seventeen out of 64 samples carried copy number alterations giving a detection rate of 26.5%. Ten of these represent benign or variables of unknown significance, giving a diagnostic capacity of the method to be 10.9%. If karyotype is performed the additional diagnostic capacity of the method is 5.1% (3/59). This study indicates the ability of array CGH to identify chromosomal abnormalities which cannot be detected during routine prenatal cytogenetic analysis, therefore increasing the overall detection rate. In addition a thorough review of the literature is presented.
Figures



References
-
- Steele MW, Breg WR., Jr. Chromosome analysis of human amniotic-fluid cells. The Lancet. 1966;1(7434):383–385. - PubMed
-
- Mohr J. Foetal genetic diagnosis: development of techniques for early sampling of foetal cells. Acta pathologica et microbiologica Scandinavica. 1968;73(1):73–77. - PubMed
-
- Leung WC, Lao TT. Rapid aneuploidy testing, traditional karyotyping, or both? The Lancet. 2005;366(9480):97–98. - PubMed
-
- Lichtenbelt KD, Knoers NV, Schuring-Blom GH. From karyotyping to array-CGH in prenatal diagnosis. Cytogenetics and Genome Research. 2011;135(3-4):241–250. - PubMed
-
- Coppinger J, Alliman S, Lamb AN, Torchia BS, Bejjani BA, Shaffer LG. Whole-genome microarray analysis in prenatal specimens identifies clinically significant chromosome alterations without increase in results of unclear significance compared to targeted microarray. Prenatal Diagnosis. 2009;29(12):1156–1166. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
