

Case of autoimmune hepatitis with markedly enlarged hepatoduodenal ligament lymph nodes
- PMID: 23555173
- PMCID: PMC3607761
- DOI: 10.3748/wjg.v19.i11.1834
Case of autoimmune hepatitis with markedly enlarged hepatoduodenal ligament lymph nodes
Abstract
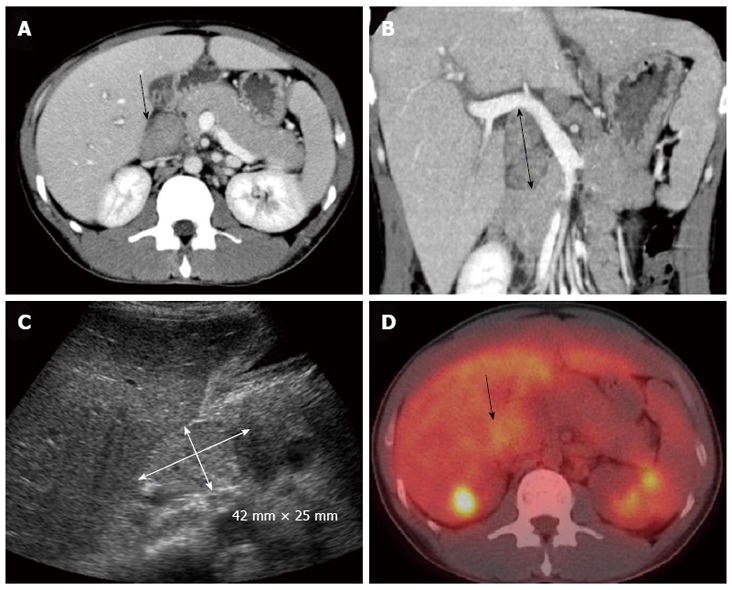
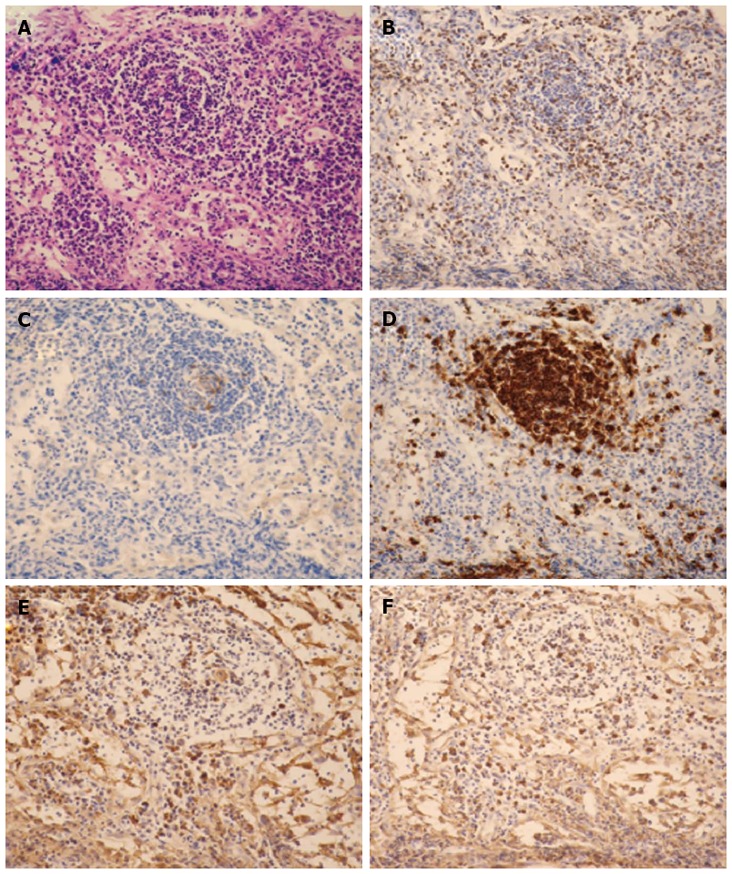
Autoimmune hepatitis (AIH) is a necroinflammatory liver disease of unknown etiology. The disease is characterized histologically by interface hepatitis, biochemically by increased aspartate aminotransferase and alanine aminotransferase levels, and serologically by increased autoantibodies and immunoglobulin G levels. Here we discuss AIH in a previously healthy 37-year-old male with highly elevated serum levels of soluble interleukin-2 receptor and markedly enlarged hepatoduodenal ligament lymph nodes (HLLNs, diameter, 50 mm). Based on these observations, the differential diagnoses were AIH, lymphoma, or Castleman's disease. Liver biopsy revealed the features of interface hepatitis without bridging fibrosis along with plasma cell infiltration which is the typical characteristics of acute AIH. Lymph node biopsy revealed lymphoid follicles with inflammatory lymphocytic infiltration; immunohistochemical examination excluded the presence of lymphoma cells. Thereafter, he was administered corticosteroid therapy: after 2 mo, the enlarged liver reached an almost normal size and the enlarged HLLNs reduced in size. We could not find AIH cases with such enlarged lymph nodes (diameter, 50 mm) in our literature review. Hence, we speculate that markedly enlarged lymph nodes observed in our patient may be caused by a highly activated, humoral immune response in AIH.
Keywords: Autoimmune hepatitis; Corticosteroid; Hepatoduodenal ligament lymph nodes; Hepatomegaly; Humoral immune response.
Figures



References
-
- Czaja AJ, Manns MP. Advances in the diagnosis, pathogenesis, and management of autoimmune hepatitis. Gastroenterology. 2010;139:58–72.e4. - PubMed
-
- Manns MP, Czaja AJ, Gorham JD, Krawitt EL, Mieli-Vergani G, Vergani D, Vierling JM. Diagnosis and management of autoimmune hepatitis. Hepatology. 2010;51:2193–2213. - PubMed
-
- Kogan J, Safadi R, Ashur Y, Shouval D, Ilan Y. Prognosis of symptomatic versus asymptomatic autoimmune hepatitis: a study of 68 patients. J Clin Gastroenterol. 2002;35:75–81. - PubMed
-
- Feld JJ, Dinh H, Arenovich T, Marcus VA, Wanless IR, Heathcote EJ. Autoimmune hepatitis: effect of symptoms and cirrhosis on natural history and outcome. Hepatology. 2005;42:53–62. - PubMed
-
- Kessler WR, Cummings OW, Eckert G, Chalasani N, Lumeng L, Kwo PY. Fulminant hepatic failure as the initial presentation of acute autoimmune hepatitis. Clin Gastroenterol Hepatol. 2004;2:625–631. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
