

Changing patterns in place of cancer death in England: a population-based study
- PMID: 23555201
- PMCID: PMC3608543
- DOI: 10.1371/journal.pmed.1001410
Changing patterns in place of cancer death in England: a population-based study
Abstract
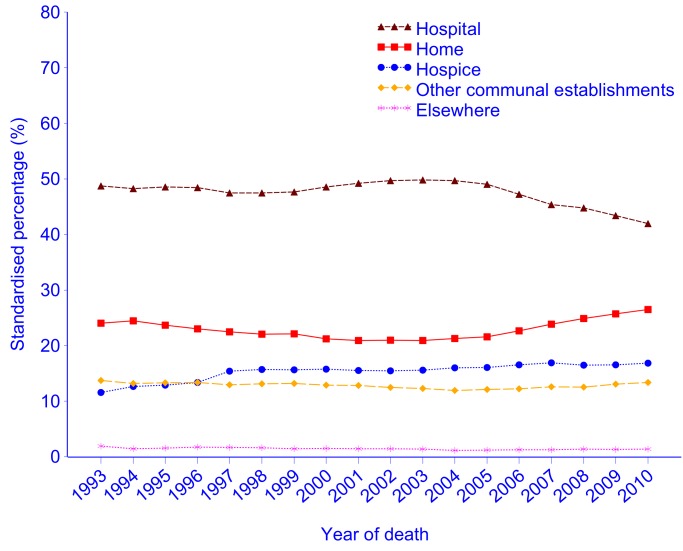
Background: Most patients with cancer prefer to die at home or in a hospice, but hospitals remain the most common place of death (PoD).This study aims to explore the changing time trends of PoD and the associated factors, which are essential for end-of-life care improvement.
Methods and findings: The study analysed all cancer deaths in England collected by the Office for National Statistics during 1993-2010 (n = 2,281,223). Time trends of age- and gender-standardised proportion of deaths in individual PoDs were evaluated using weighted piecewise linear regression. Variables associated with PoD (home or hospice versus hospital) were determined using proportion ratio (PR) derived from the log-binomial regression, adjusting for clustering effects. Hospital remained the most common PoD throughout the study period (48.0%; 95% CI 47.9%-48.0%), followed by home (24.5%; 95% CI 24.4%-24.5%), and hospice (16.4%; 95% CI 16.3%-16.4%). Home and hospice deaths increased since 2005 (0.87%; 95% CI 0.74%-0.99%/year, 0.24%; 95% CI 0.17%-0.32%/year, respectively, p<0.001), while hospital deaths declined (-1.20%; 95% CI -1.41 to -0.99/year, p<0.001). Patients who died from haematological cancer (PRs 0.46-0.52), who were single, widowed, or divorced (PRs 0.75-0.88), and aged over 75 (PRs 0.81-0.84 for 75-84; 0.66-0.72 for 85+) were less likely to die in home or hospice (p<0.001; reference groups: colorectal cancer, married, age 25-54). There was little improvement in patients with lung cancer of dying in home or hospice (PRs 0.87-0.88). Marital status became the second most important factor associated with PoD, after cancer type. Patients from less deprived areas (higher quintile of the deprivation index) were more likely to die at home or in a hospice than those from more deprived areas (lower quintile of the deprivation index; PRs 1.02-1.12). The analysis is limited by a lack of data on individual patients' preferences for PoD or a clinical indication of the most appropriate PoD.
Conclusions: More efforts are needed to reduce hospital deaths. Health care facilities should be improved and enhanced to support the increased home and hospice deaths. People who are single, widowed, or divorced should be a focus for end-of-life care improvement, along with known at risk groups such as haematological cancer, lung cancer, older age, and deprivation. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO Media centre (2013) Cancer: Fact sheet No 297. Accessed 26 January 2013. Available: http://www.who.int/mediacentre/factsheets/fs297/en/index.html.
-
- Gomes B, Higginson IJ, Calanzani N, Cohen J, Deliens L, et al. (2012) Preferences for place of death if faced with advanced cancer: a population survey in England, Flanders, Germany, Italy, the Netherlands, Portugal and Spain. Ann Oncol 23: 2006–2015. - PubMed
-
- Mitchell AJ, Chan M, Bhatti H, Halton M, Grassi L, et al. (2011) Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol 12: 160–174. - PubMed
-
- Lindqvist O, Tishelman C, Hagelin CL, Clark JB, Daud ML, et al. (2012) Complexity in non-pharmacological caregiving activities at the end of life: an international qualitative study. PLoS Med 9: e1001173 doi:10.1371/journal.pmed.1001173. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
