

Primary aortic infections and infected aneurysms
- PMID: 23555384
- PMCID: PMC3595813
- DOI: 10.3400/avd.AVDctiia09001
Primary aortic infections and infected aneurysms
Abstract
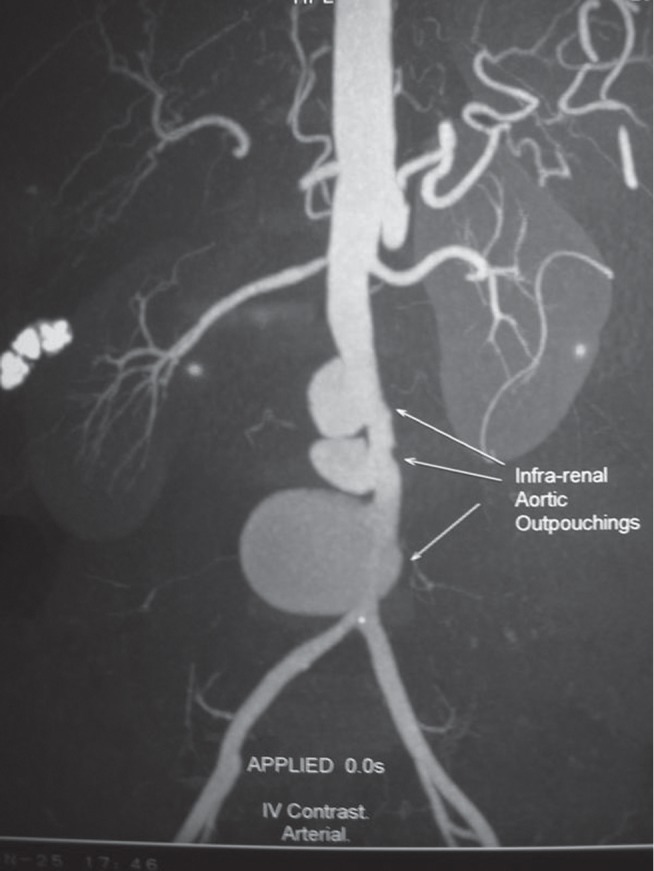
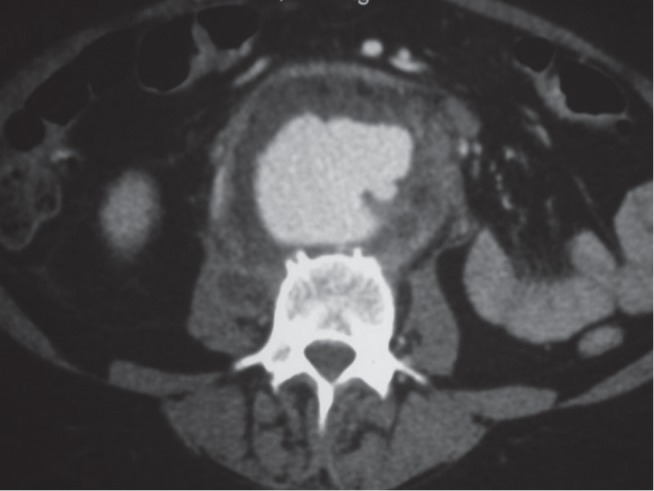
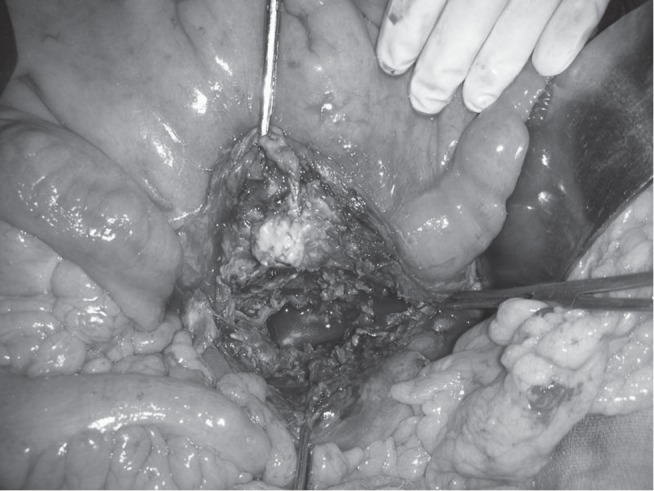
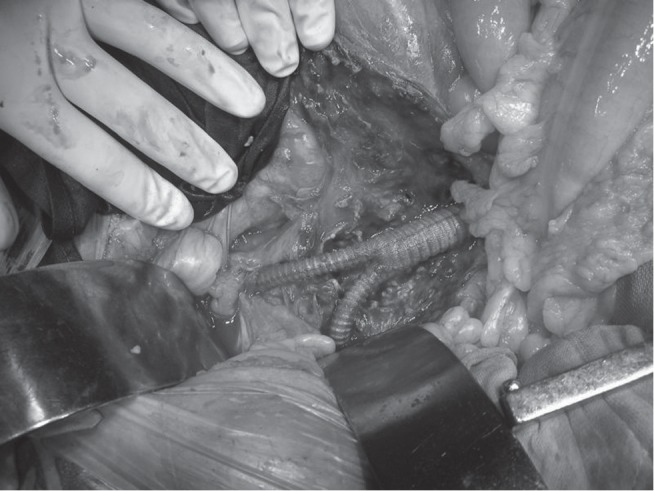
Primary infections of the aorta and infected aortic aneurysms are rare and are life threatening. Most of them are due to bacterial infection occurring in an atheromatous plaque or a pre existing aneurysm during bacteremia. Rarely spread from a contiguous septic process may be the cause. The reported hospital mortality ranges from 16-44%. Gram positive bacteria are still the most common causative organisms. More recently, Gram negative bacilli are seen increasingly responsible. The mortality rate is higher for the Gram negative infection since they most often cause supra renal aneurysms and are more prone for rupture. Best results are achieved by appropriate antibiotics and aggressive surgical treatment. Excision of the infected aneurysm sac as well as surrounding tissue and in situ reconstruction of aorta is the preferred treatment. Pedicled omental cover also helps to reduce infection. Long term antibiotic is needed to prevent reinfection. Mortality is high for those who undergo emergency operation, with advanced age and for nonsalmonella infection.
Keywords: aorta; aortitis; mycotic aneurysm; pseudo aneurysm.
Figures
References
-
- Reddy DJ, Weaver MR. Chap 108: Infected aneurysms. Rutherford Vascular Surgery, Elsevier Saunders, Philadelphia: 6th edition2006; 1581–96
-
- Brown SL, Busutill RW, Baker JD, Machleder HI, Moore WS, Barker WF. Bacteriologic and surgical determinants of survival in patients with mycotic aneurysms. J Vasc Surg. 1984; 1: 541. - PubMed
-
- Canaud L, Marzelle J, Bassinet L, Carrié AS, Desgranges P, Becquemin JP. Tuberculous aneurysms of the abdominal aorta. J Vasc Surg. 2008; 48: 1012–6 - PubMed
-
- Reddy DJ, Shepard AD, Evans JR, Wright DJ, Smith RF, Ernst CB. Management of infected aortoiliac aneurysms. Arch Surg. 1991; 126: 873–8 - PubMed
LinkOut - more resources
Full Text Sources