

Cardiac and Aortic Reoperation for Patients with Functional Grafts after CABG
- PMID: 23555468
- PMCID: PMC3614397
- DOI: 10.3400/avd.oa.11.00039
Cardiac and Aortic Reoperation for Patients with Functional Grafts after CABG
Abstract
Objective: Late cardiac and aortic reoperation after CABG is indispensable for patients with atherosclerotic disease, but reoperations are still associated with high morbidity rates.
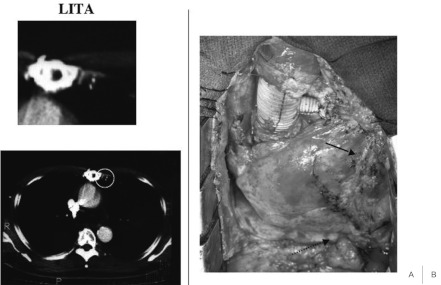
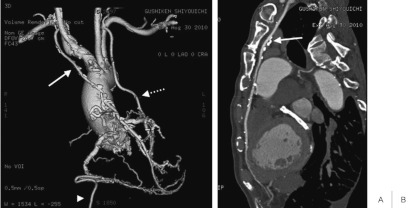
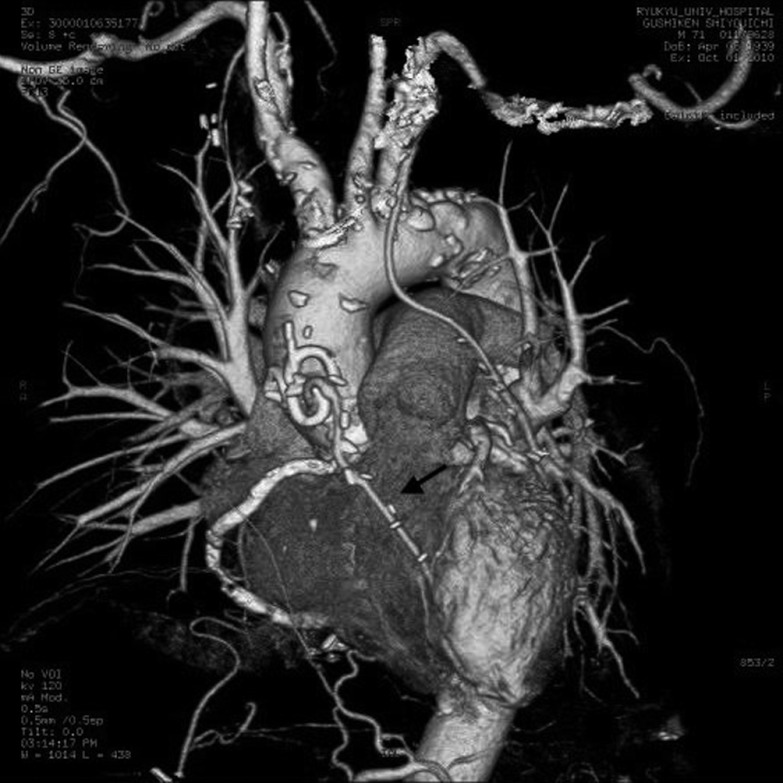
Patients and methods: Between January 2002 and December 2010, 459 patients underwent coronary artery bypass grafting. Six patients (males; mean age, 65.0 ± 5.7 years) with previous arterial bypass grafts (mean, 2.8 ± 1.2 per patient) required reoperation for cardiac and aortic disease (3, valvular disease; 3, acute type I aortic dissection) during long-term follow-up. The mean interval between the initial operation and reoperation was 5.4 ± 2.0 years. Grafts visualized by preoperative enhanced computed tomography were harvested as pedicles and clamped for myocardial protection. The total arch or ascending aorta was replaced in three patients. The aortic valve was replaced in two patients, and the aortic and mitral valves were replaced in one.
Results: Durations for surgery, total cardiopulmonary bypass, and cardiac ischemia were 611.5 ± 172.6, 223.2 ± 88.4, and 133.4 ± 58.0 minutes, respectively. Perioperative myocardial infarction did not develop, and all patients recovered uneventfully with no neurological deficits.
Conclusion: Bypass grafts should be preoperatively visualized and carefully exposed. Cardiac damage must be avoided during reoperation after coronary artery bypass grafting.
Keywords: aortic dissection; cardiac reoperation; coronary artery bypass grafting; internal thoracic artery.
Figures
Similar articles
-
Results of late-onset type A aortic dissection after previous cardiac surgery: Does prior coronary artery bypass grafting affect survival?Turk Gogus Kalp Damar Cerrahisi Derg. 2018 Jan 9;26(1):1-7. doi: 10.5606/tgkdc.dergisi.2018.14683. eCollection 2018 Jan. Turk Gogus Kalp Damar Cerrahisi Derg. 2018. PMID: 32082704 Free PMC article.
-
Reoperations on the aortic root and ascending aorta.Ann Thorac Surg. 1997 Oct;64(4):986-92. doi: 10.1016/s0003-4975(97)00626-7. Ann Thorac Surg. 1997. PMID: 9354515
-
Mitral valve surgery after previous CABG with functioning IMA grafts.Ann Thorac Surg. 1999 Dec;68(6):2243-7. doi: 10.1016/s0003-4975(99)01120-0. Ann Thorac Surg. 1999. PMID: 10617010
-
Reusing the patent internal mammary artery as a conduit in redo coronary artery bypass surgery.Interact Cardiovasc Thorac Surg. 2016 Mar;22(3):346-50. doi: 10.1093/icvts/ivv338. Epub 2015 Dec 15. Interact Cardiovasc Thorac Surg. 2016. PMID: 26669852 Free PMC article. Review.
-
Aortic valve replacement after previous coronary artery bypass grafting.Ann Thorac Surg. 1996 Nov;62(5):1424-30. doi: 10.1016/0003-4975(96)00635-2. Ann Thorac Surg. 1996. PMID: 8893579 Review.
References
LinkOut - more resources
Full Text Sources