

Quantitative susceptibility mapping differentiates between blood depositions and calcifications in patients with glioblastoma
- PMID: 23555565
- PMCID: PMC3605431
- DOI: 10.1371/journal.pone.0057924
Quantitative susceptibility mapping differentiates between blood depositions and calcifications in patients with glioblastoma
Abstract
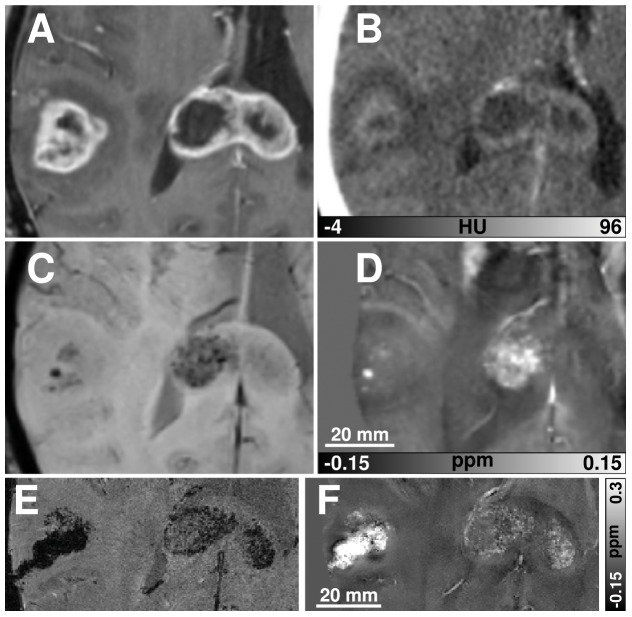
Objectives: The application of susceptibility weighted imaging (SWI) in brain tumor imaging is mainly used to assess tumor-related "susceptibility based signals" (SBS). The origin of SBS in glioblastoma is still unknown, potentially representing calcifications or blood depositions. Reliable differentiation between both entities may be important to evaluate treatment response and to identify glioblastoma with oligodendroglial components that are supposed to present calcifications. Since calcifications and blood deposits are difficult to differentiate using conventional MRI, we investigated whether a new post-processing approach, quantitative susceptibility mapping (QSM), is able to distinguish between both entities reliably.
Materials and methods: SWI, FLAIR, and T1-w images were acquired from 46 patients with glioblastoma (14 newly diagnosed, 24 treated with radiochemotherapy, 8 treated with radiochemotherapy and additional anti-angiogenic medication). Susceptibility maps were calculated from SWI data. All glioblastoma were evaluated for the appearance of hypointense or hyperintense correlates of SBS on the susceptibility maps.
Results: 43 of 46 glioblastoma presented only hyperintense intratumoral SBS on susceptibility maps, indicating blood deposits. Additional hypointense correlates of tumor-related SBS on susceptibility maps, indicating calcification, were identified in 2 patients being treated with radiochemotherapy and in one patient being treated with additional anti-angiogenic medication. Histopathologic reports revealed an oligodendroglial component in one patient that presented calcifications on susceptibility maps.
Conclusions: QSM provides a quantitative, local MRI contrast, which reliably differentiates between blood deposits and calcifications. Thus, quantitative susceptibility mapping appears promising to identify rare variants of glioblastoma with oligodendroglial components non-invasively and may allow monitoring the role of calcification in the context of different therapy regimes.
Conflict of interest statement
Figures





References
-
- Wen PY, Kesari S (2008) Malignant gliomas in adults. N Engl J Med 359: 492–507. - PubMed
-
- Wong ET, Hess KR, Gleason MJ, Jaeckle KA, Kyritsis AP, et al. (1999) Outcomes and prognostic factors in recurrent glioma patients enrolled onto phase II clinical trials. J Clin Oncol 17: 2572–2578. - PubMed
-
- Sehgal V, Delproposto Z, Haddar D, Haacke EM, Sloan AE, et al. (2006) Susceptibility-weighted imaging to visualize blood products and improve tumor contrast in the study of brain masses. J Magn Reson Imaging 24: 41–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
