

Chemotherapy plus best supportive care versus best supportive care in patients with non-small cell lung cancer: a meta-analysis of randomized controlled trials
- PMID: 23555583
- PMCID: PMC3603584
- DOI: 10.1371/journal.pone.0058466
Chemotherapy plus best supportive care versus best supportive care in patients with non-small cell lung cancer: a meta-analysis of randomized controlled trials
Abstract
Background: The use of chemotherapy has been proposed to increase the effectiveness of best supportive care (BSC) in patients with non-small cell lung cancer (NSCLC). Previous trials reported inconsistent findings regarding the efficacy and safety of chemotherapy on overall survival (OS) and treatment-related mortality. We performed a systematic review and meta-analysis to evaluate the effects of chemotherapy plus BSC versus BSC alone on survival of patients with NSCLC.
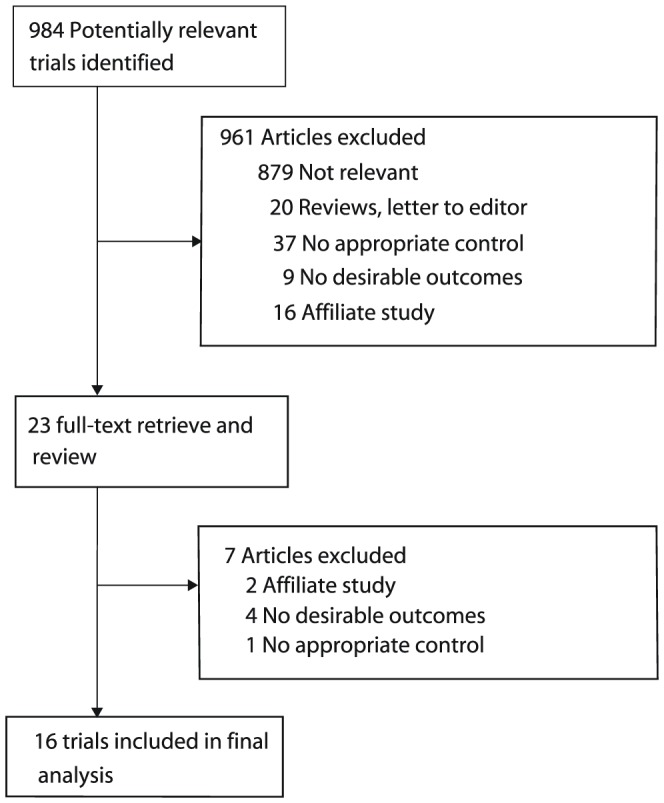
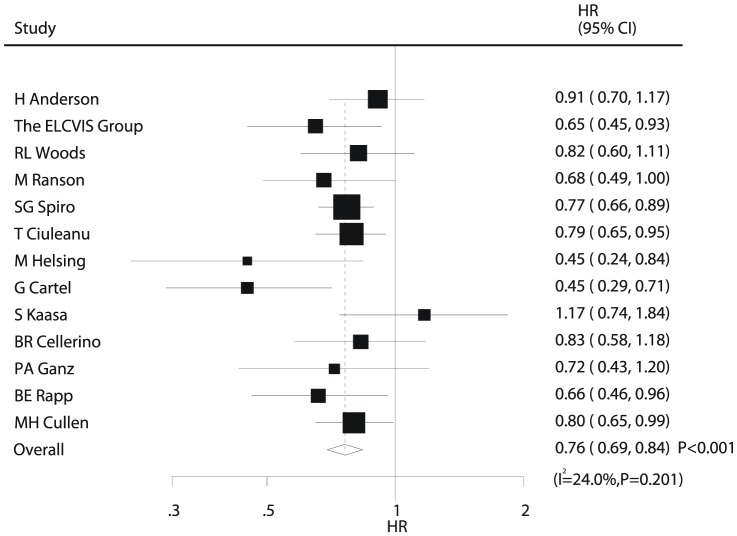
Methodology and principal findings: We systematically searched PubMed, EmBase, and the Cochrane Central Register of Controlled Trials for relevant literature. All eligible studies included patients with NSCLC who had received chemotherapy and BSC or BSC alone. All eligible studies measured at least 1 of the following outcomes: OS or treatment-related mortality. Overall, patients that received chemotherapy plus BSC had significant longer OS than those that received BSC alone (HR, 0.76; 95%CI, 0.69-0.84; P<0.001). Additionally, chemotherapy plus BSC as compared to BSC alone resulted in a 28% RR reduction (95%CI: 12-40; P = 0.001) in 6-month mortality, 11% RR reduction (95%CI: 8-15; P<0.001) in 12-month mortality, and 5% RR reduction (95%CI: 1-8; P = 0.02) in 2-year mortality. Toxicity was greater in patients that received chemotherapy plus BSC.
Conclusion/significance: Chemotherapy plus BSC increased the OS and reduced the 6-month, 12-month, and 2-year mortality of NSCLC patients.
Conflict of interest statement
Figures


References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, et al. (2009) Cancer statistics, 2009. CA Cancer J Clin 59: 225–249. - PubMed
-
- Wingo PA, Cardinez CJ, Landis SH (2003) Long-term trends in cancer mortality in the United States, 1930–1998. Cancer 97: 3133–3275. - PubMed
-
- Rudd R (1991) Chemotherapy in the treatment of non-small cell lung cancer. Respiratory Disease in Practice 7 6: 12–4.
-
- Aisner J, Hansen HH (1981) Commentary: Current status of chemotherapy for non-small cell lung cancer. Cancer Treat Rep 65: 979–86. - PubMed
-
- Hoffman PC, Bitran JD, Golomb HM (1983) Chemotherapy of metastatic non-small cell bronchogenic carcinoma. Semin Oncol 10: 111–122. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
